")
Back Knee alias Genu Recurvatum
 This is surely the most misunderstood topic in discussing walking and walking pathology. First the terms:
This is surely the most misunderstood topic in discussing walking and walking pathology. First the terms:
Genu = Knee.
Recurvatum = bent backward.
Let's get the bottom line right up front.
NOT ALL BACK KNEE IS BAD!
We have to start with that. Why? Because over and over and over we see the identification of back knee glued right onto a huge treatment. In fact, certain treatments for other walking conditions have built-in back knee prevention which may well be inappropriate. The treatment plan includes portions to prevent back knee which may actually be useful, were it present.
Above we see the real thing. That is quite bad and treatment is complex. However, small back ankles that occur in walking get painted with the same brush - and ought not.
It all has to do with control mechanisms and momentum.
First we have the body mass whose balance center is in the pelvis. That mass in walking has considerable momentum (ever walk into a wall in the dark? BOOM!).
* the thigh
* the knee joint (with the knee cap in front)
* the shin
* the foot
WALKING: In walking there is momentum. That is, if you stop the thigh, the pelvis will lurch forward at the hip. If you stop the knee, the femur will continue ahead and get tilted ahead of the shin (back knee) and the pelvis will lurch past the hip by flexing at the hip. If you stop the shin, you also stop the knee so you get a back knee and pelvis lurch. If you only stop the toe area, the heel rises as the shin tilts suddenly forward. The knee may bend depending on the position of the body above. If the stopped toe is behind the body when the stoppage happens, then you fall - plop. That's called "stubbing" your toe (arresting its flight behind the body). If you stop the toe well ahead of the body, that's called braking - screeeeeech. Stop.
See? Momentum. The big MO. Either you are in position to use it, break it, or fall (victim) to it.
Picture monkeys swinging on vines. If the monkey is hanging still on one vine, grabbing a near vine will do very little. No momentum. Swinging through the trees requires that the momentum of one swing not be lost as the next vine is grabbed. Position matters.
The swing leg is a pendulum with momentum. The stance leg is also a vertical pendulum (like a metronome or ground punching bag). The two must be in sync or the energy transfer - as demanding as the monkey going from vine to vine - is defective and energy is lost. That is you stop, or a portion of you stops, as some other portion keeps going. In our discussion of walking, energy and momentum was stressed. In fact "walking" has been refined in its definition by the senior group member as only referring to gait in which momentum is utilized. Muscles do a whole different thing if momentum is at work. If not, if each body part has to be muscularly positioned in its entirety - that called "stepping". Walking implies a seamless energy and momentum transfer from right to left to right...
STEPPING: Stepping is just a series of steps. We all use stepping when we do that silly graduation march (march to somebody else's drummer), climb stairs, or walk in deep snow. If the pendulums (our legs) are dampened, robbed of momentum by resisted movement, we must step. A very good name for such gait is stair climbing. As our mechanism of momentum conservation fails on stairs, we experience stepping on - steps. When you see a child walking, but the walk has a look of stair climbing, that's stepping. The root cause is inability to synchronize the seamless transfer of momentum from one limb to the other.
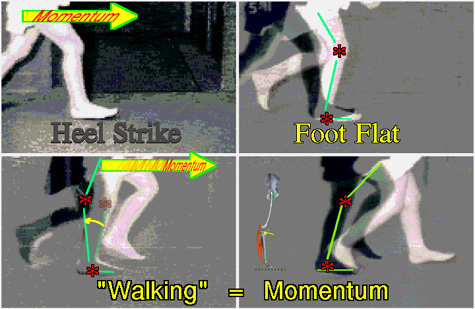 As the heel strikes the extended leg (thigh + shin) flexes as the body center passes above the ankle.
As the heel strikes the extended leg (thigh + shin) flexes as the body center passes above the ankle.
The shortening of the shin-femur linkage by knee flexion allows the momentum above to travel a more horizontal path (less against gravity).
After foot flat, the ankle stiffens. It essentially becomes rigid with the shin forward off vertical by about 10 to 15 degrees. Momentum against the stiff ankle causes the heel to rise as the ball of the foot becomes the rolling point.
So notice, the knee is ahead of the ankle when the hip is above the ankle and the momentum is forward the ankle when the ankle stiffens. That rolls the foot over the metatarsals as the thigh-shin linkage straightens out again to keep momentum on a near level course.
If the ankle is SLOW in allowing the shin to come forward (forget what its range of motion is, this has to be speedy or it doesn't count) - again - if the ankle is SLOW in allowing the shin to come forward, then the thigh and pelvis pass it up. Boing! Recurvatum. Back knee. See the stick figures in the images for back knee. A tight calf muscle or Achilles mechanism will cause back knee because it holds the shin bone back. This backward drive against the knee from a resisted forward roll of the ankle gets its force from the ground as the foot becomes one with the ground. This the the origin of the term ground reaction.
That's bad. Right? Yes. Why? It robs energy and is tiring and involves a huge energy slam at the knee which can damage the knee over time.
mpg-1 =>
|

showing ground reaction back knee
[ if you don't have MPEG play capability- get it- reason : file size & quality ]
[ if your viewer allows it, step through the sequence slowly to see it better ]
What are we seeing here? A youngster slamming knees back on every step.
Recurvatum that follows weight acceptance on the foot is very forceful.
But there are other kinds of back knee. Look at the lower right square of the composite 4-part image above. In normal walking there is an instant where the hind leg is on toe and the forward leg is on heel only. Two points.
Children with ataxia (balance loss) or with sensory loss, may feel insecure in transferring weight to the forward stance leg before they are sure it is solidly secured. They will keep the rear foot fully planted (foot flat) until the body above shifts over the forward leg with that foot also fully flat. The rear leg will have a mild back knee because the heel has not risen. This type of back knee is not under landing forces (compression) but under distractive forces (take off). It is benign and needed for compensatory balance. Leave it. There is some energy loss, but how much depends on just how long the hesitation lasts. Typically, such children are taking huge steps which exaggerates the look.
But what if the youngster simply cannot control momentum? There may be insufficient sensory control or much too slow reaction, or the math of walking is just not there. Then what?
Then stepping. Stepping is gait without momentum mechanisms. Each action is performed in its entirety by discrete muscle effort and not pulled into existence or magnified by momentum. When we walk slowly in a crowd, leaving the movies, we step. Without momentum we must completely shift our weight over each leg in turn - we sway side to side. The flexed transitional postures of walking are inherently unstable. If we had to stay in such a posture without the momentum, we would be exhausted.
Steppers, in flexed postures, will burn out. They require islands of stability with each step to replenish muscle energy. Small back knee postures are inherently stable. They work well for steppers but ruin walkers. We may well design in some inherent knee stability for a youngster who lacks the control mechanisms required of walking.
PROBLEMS?
Here's one problem. Some steppers may eventually improve so as to become potential walkers. We can't let the locking strategy run amok. Think of it as training wheels on a bike. We need a way to remove that feature if skill appears.
Another common problem is that we have determined reasonable control sensitivity in a child who has never walked (real walking, not stepping). The hamstrings are way way tight but the calf muscles are only a wee bit tight. If we optimize hamstring length and flexibility in the absence of secure skill, then the insecurity of low skill will tend to cause antigravity actions to overshoot into extension (at the ankle). This will produce a ground reaction back knee. A clear cut example is when the child back knee walks when not holding on but then does not back knee when using a walker or when holding someone's hand. Here, fear => fixing (unmeasured antigravity oomph) which => recurvatum. Treatment: Use the AFO!!! and make sure it is set to 10 to 15 degrees forward tilted when the SHOE is flat to the ground.
Fixing may also bring in quadriceps. In that case, even with the AFO, the foot will hang on the heel with the ball of the foot off the ground. Moving the heel back on the shoe counters this. Use this easy remedy until the fear factor subsides as will the back knee.
A long STIFF toe plate on a foot brace will make metatarsal head (ball of foot) roll over impossible and produce back knee, exaggerated in or out turn, and hop off gait. Stiff toe plates are OFTEN prescribed so as to act as a therapy ground reaction to stretch the Achilles. It is not easily steered to just the Achilles. So what is aimed at the Achilles may well be blasting away at the knee as back knee. Also, decide, is walking to be therapy or walking? If walking is to be walking, then the toe plate must flex almost as if it were not there.
One of the nice things about selective percutaneous myofascial lengthening, is that we have a handle on every single aspect of this phenomenon. It just takes a bit of practice to get it right and to lose fear driven over reaction.