|
|
||||||||||||||||||||

|
|

|
Just deep to where the outcropping thumb muscles of the thumb emerge, the pronator teres inserts on the radius at the outer edge. When spastic, it has very strong posture from which to sustain pronation. Another pronator (pronator teres) is deep under that wrist band right on the two bones beneath the passing tendons. It is also a strong pronating force in spasticity. The biceps is often difficult at the same time also attaching to the radius. However, the biceps is a supinator. That's another reason to go proximal with long term biceps procedures so as to not lose the supination.
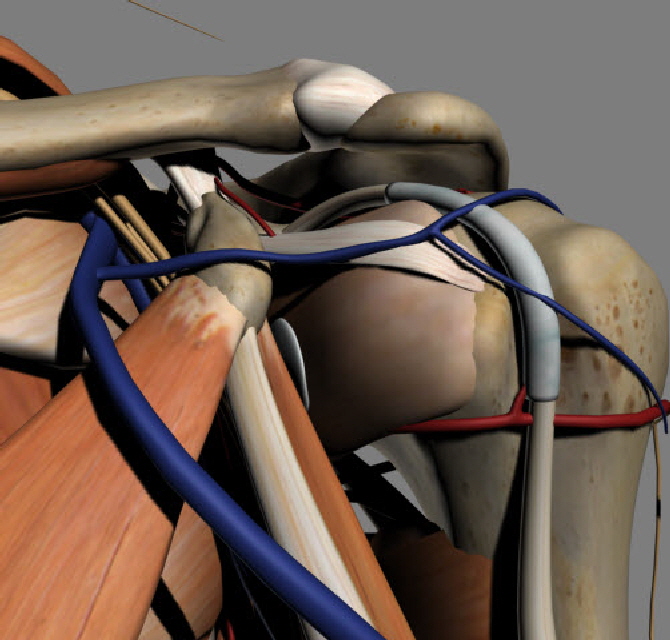
So the triceps long head is posterior to both these muscles. The area of the upper arm typically called "the Biceps" is actually a stack of muscles. The biceps runs from the radius in the proximal forearm to the top of the glenoid (cup of the shoulder blade, the actual shoulder joint for the big stuff). It also sends a portion to the coracoid - a finger of bone pointing forward from the top of the scapula.
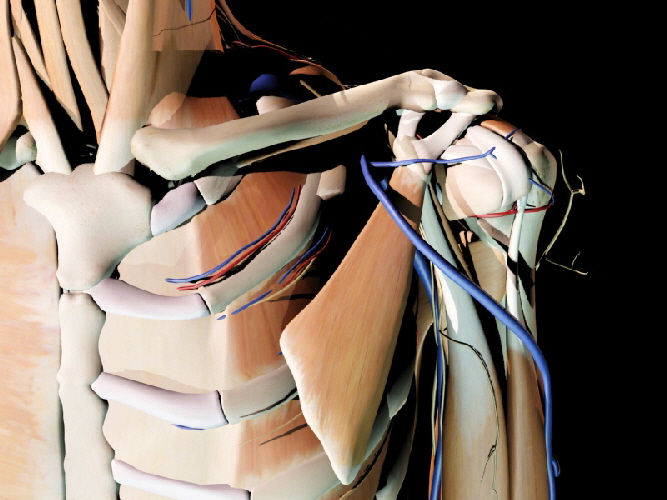
The AC joint is the joint between the clavicle (C) and the Acromion (A). The bursa beneath the acromion is the one that gets most commonly needled in 'bursitis'
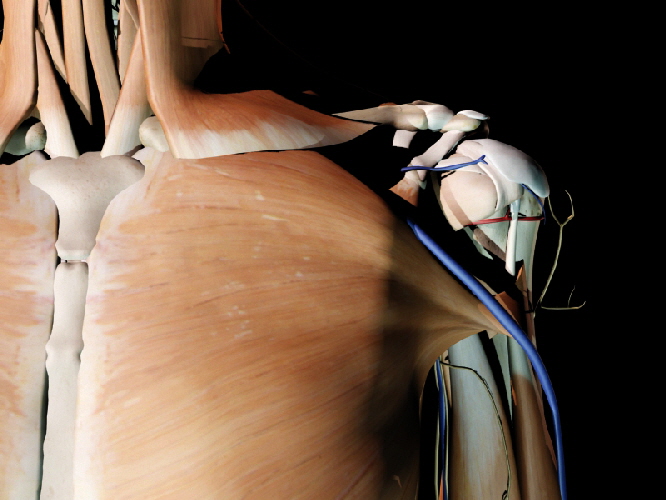
Notice how the pectoralis major upper edge attaches at the bottom of the humeral attachment. It's lower muscular edge goes to the top of the humeral attachment. This half twist is very common to tendon all about the body and enriches the action of the muscle through the arc and maintaining a more even tension through the sweet spot of its usual usage.
The coracoid process is a finger of bone from the scapula jutting forward. From its bottom hang muscles (pec. minor, coracobrachialis, biceps). From its top a crown of thorns - well ligaments that can FEEL thorny if you have impingement syndrome. The impingement syndrome is the ouchy condition often attributed to the humerus's big bump (greater tuberosity = big bump) having difficulty passing under the acromion. The bursa is a slippery tissue to help that glide. The AC joint often collects some debris from that grind and gets blamed for the lack of space. Like blaming the floor for
collecting saw dust - OK, OK, so I am NOT a believer in this. Many shoulders are getting scoped to chew away the under-surface of the acromion and the AC joint. AND IT WORKS!!!!!!!!
What does this have to do with us? This isn't sports medicine here. Well take a look at a polio patient doing a discus throw of their folded wheel chair into a truck or car trunk. Folks with lower limb disabilities often use their arms for more things and more energetically. Then they get wrong diagnoses made. Shoulder pain can be neck ruptured disc, thoracic outlet compression of nerves (& or vessels), coracoid related ligament impingement of the shoulder cuff and occasionally AC joint impingement.
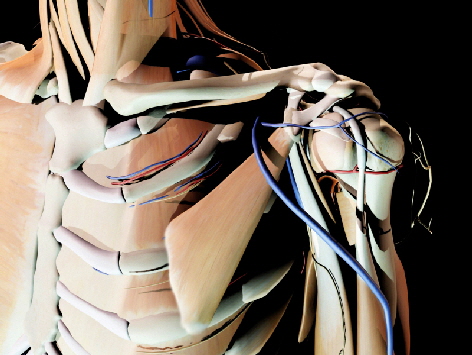
Would you believe there is a syndrome with squeezing the artery & nerve in the quadrilateral space? Always bet yes to this type question as every space that passes something has a syndrome that happens when the passage is tight (carpal tunnel syndrome is just one on many). Tenderness in this spot to a probing finger when some unconditioned event is followed by gnawing deep and curiously low (not AC) zapping discomfort.
As he glenohumeral ligament moves WITH the humerus it is not an impingement source. It can be a victim. It may well be torn when shoulders dislocate. Indeed the nerve to the subscapularis can be stretched to the point of being put out of commission (maybe 25% of the time?). It is thought to recover, though, if you wait and so some joint laxity can 'heal' by doing nothing (nerve comes back). High five. Notice the long trek of the biceps tendon through the bicipital groove heading for the top of the glenoid. The sheath lubricates it there and reduces wear friction.
The omohyoid muscle can be under formed and sometimes be made of BONE. The wing bone (scapula) will then be on a stiff tether and typically ride high. In certain cases, the entire shoulder unit may be under developed. In evolution or comparative anatomy, the vertebrates body plan is a long string of repeating units (such as vertebrae and the go-withs) bracketed on each side at intervals by 'girdles. These girdles are typically three bone units with goodies than can extend out. So pelvis of three fused bones per side with legs and in people another girdle at the shoulders as a scapula with arms that stick out. There is a nearly 1:1 correlation between muscles in the arms and those in the legs. Nice design. But as embryonic overall patterns get stretched out here & there some may fail. So if the shoulder girdle gets too attached it may follow the neck & head growth with the shoulder winding up behind the ear. There are degrees of this from the rare Sprengel's deformity which may also have the omohyoid BONE and also may be associated with other abnormal neck bone formations (Klippel-Feil syndrome) to the very very common slight and why are you looking so hard at it teeny difference in height of the scapulae. No, it is NOT scoliosis. Very common school screening misdiagnoses of scoliosis comes from this slight asymmetry. Here is an example of how the linkage pattern for a muscle can be used (or reduced) to alter neurologic response. The biceps - as its name tells you - has two origins. The one to the coracoid process is well off center and like a cam will tug more as the arm dangles and body position changes. If the biceps is too sensitive and spastic, eliminating this origin removes much of the self stimulation that comes from minor posture changes.
|
 Notice the latissimus inserts on the humerus in front of the long head of the triceps. This muscle is the power house of the butterfly swim stroke, pulling
strongly to pull the arm to the side of the body while rotating the arms inward (slap your thigh) and bringing the elbows slightly backward. This muscle on the
back attaching on the nearly front of the humerus is also a gymnast's key mover. The Teres major is much smaller, but attaches on the humerus just down stream
of the lat. It is as if the Teres major is just the lat portion that has origin on the scapula. By attaching further down on the humerus - further from joint center - it
gets some improved strength by the longer leverage. This also makes it a 'faster' muscle in that it travels further with the same arc.
Notice the latissimus inserts on the humerus in front of the long head of the triceps. This muscle is the power house of the butterfly swim stroke, pulling
strongly to pull the arm to the side of the body while rotating the arms inward (slap your thigh) and bringing the elbows slightly backward. This muscle on the
back attaching on the nearly front of the humerus is also a gymnast's key mover. The Teres major is much smaller, but attaches on the humerus just down stream
of the lat. It is as if the Teres major is just the lat portion that has origin on the scapula. By attaching further down on the humerus - further from joint center - it
gets some improved strength by the longer leverage. This also makes it a 'faster' muscle in that it travels further with the same arc.



|
|
 |
||||||||||||||
|
|
||||||||||||||