|
|
||||||||||||||||||||

 |
 |
|
So is it adductor pollicis brevis? No. Just adductor pollicis. A rose by any name... We will try not to get hung up in the twisted naming, but as you may want to know what it was you heard them talking about I will pepper this with the various terms and be a bit redundant.
There are kinds of muscles in the hand, grouped by their team membership. There is a compelling logic to it all but one that is amazingly organized. To allow graceful curved motion the muscles layer with some going a shorter distance and others going to the end. The ones going the long distance are deeper (unlike in the leg). So in the hand the long muscles must pass through tunnels in those that end sooner. The thumb sticks out, and so do many of the thumb muscles.
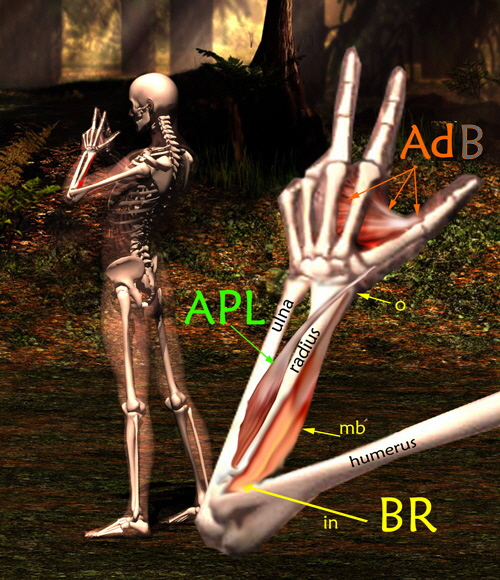
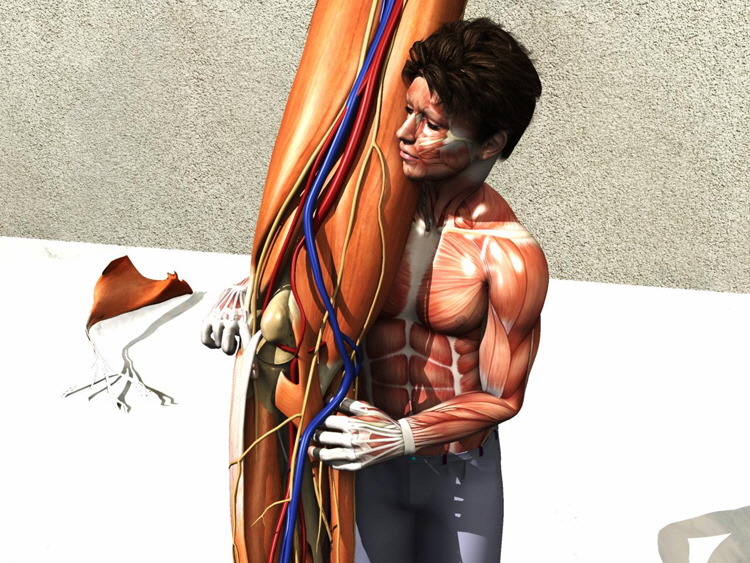
Almost to the ulnar side (side opposite the thumb) the small finger extensor gets its own sheath under the wrist band (called retinaculum and specifically the dorsal [hairy side] carpal ligament). The last sheath is the one for the ECU extensor carpi ulnaris landing at the base of the little finger metacarpal. So on top of the wrist the two sets of wrist extensors bracket the width of the wrist - the thumb EPB APL are not on top but on the side - the radial side. Here we see the wrist from the radial dorsal side and four volar views (palm side) of the forearm showing how tendons allow the muscles to act from afar in tight quarters. Get it? Puppets. Fingers are puppets. The big work is in the forearm.
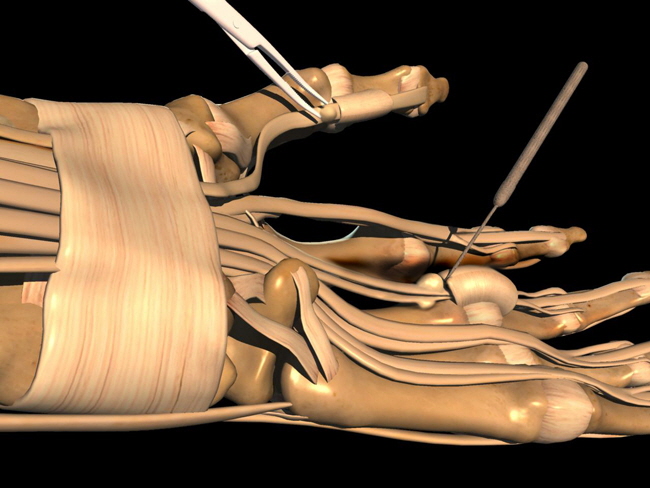
Those muscles that are in the hand itself are called the intrinsic muscles of the hand. However two bunches of those get their own names and so are not typically intrinsics as such. These are the THENAR (thumb base muscles) and the HYPOTHENAR muscles (base of little finger). Notice that the ADDUCTOR of the thumb (Adductor pollicis or AdP tempting to add B) originates from the metacarpal of the third finger. The Abductor pollicis (AbP) isn't seen as it is just deep to the Opponens pollicis. Whoa. Place your hand on a flat surface palm side up. Bring your thumb closed to the hand adjacent the index metacarpal. That is adduction. Relax. Now stand the thumb straight up like a tree (back of hand still flat to table). That's opposition - the beginning half of it. Now from that tree posture touch the thumb tip to the base of the fifth finger. That's the rest of opposition. There are more tunnels than those on the back of the wrist. Here we see the well known 'Carpal tunnel'. All the long finger flexors share the same tunnel on the volar (palmar) side of the wrist. The bones of the wrist - the carpal bones - are set out as a stone archway. The bottom of that arch is spanned by the transverse carpal ligament. This young fellow has his finger probing the carpal tunnel from the distal part (with local muscles removed ). We see that the 'MEDIAN NERVE' shares this tunnel to get to the hand. If the ligament thickens, then tightness here would make or numbness or tingling in the median nerve distribution (palmar side of fingers 1,2, & 3 and the radial side (thumbward side) of finger 4.
The ulnar side of the 4th finger and the whole 5th finger (both on the palmar surface) are served by the ulnar nerve which has its own private entry to the hand through Guyon's Canal (seen being probed below). Serving only that one nerve it is quite a bit smaller in diameter than the one called the carpal tunnel.
Not often thought of as tunnels At the level of the distal metacarpals hollow tunnels cover the superficial (short) finger flexor stacked on top of the long finger flexor known as the profundus (flexor digitorum profundus). It is long and deep. At the level of the first finger joint (next after the metacarpal phalangeal or MP joint) the first finger joint being called the PIP (Proximal interphalangeal), at that level . the superficial flexor tendon splits to attach to the middle phalange base. It creates a tunnel through which the profundus passes heading to the terminal phalange at the DIP - distal interphalangeal joint. See where the kid has his finger. If the tendon gets swollen here, it will rub within the tunnel and swell more and more until it gets stuck. It can pop through under tension and the finger can get stuck in flexion or in extension depending on what side of the tunnel the swelling hangs.
Here, lets grab and lift the superficialis (superficial flexor) tendons (heading to fingers 2-5, that is, index to pinky)
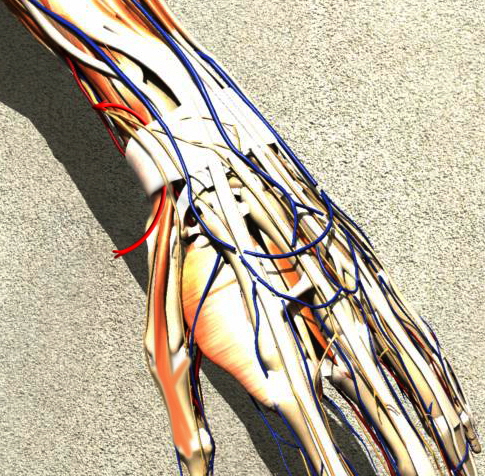
Like this, below. See the profundus tendons are below the superficialis. It had better be that way or the names would be way way off! The median nerve sits right near the surface, centered with this group. Many people do not have a Palmaris longus muscle & tendon which is even more superficial dead center and attaches to the transverse carpal ligament and palmar fascia.
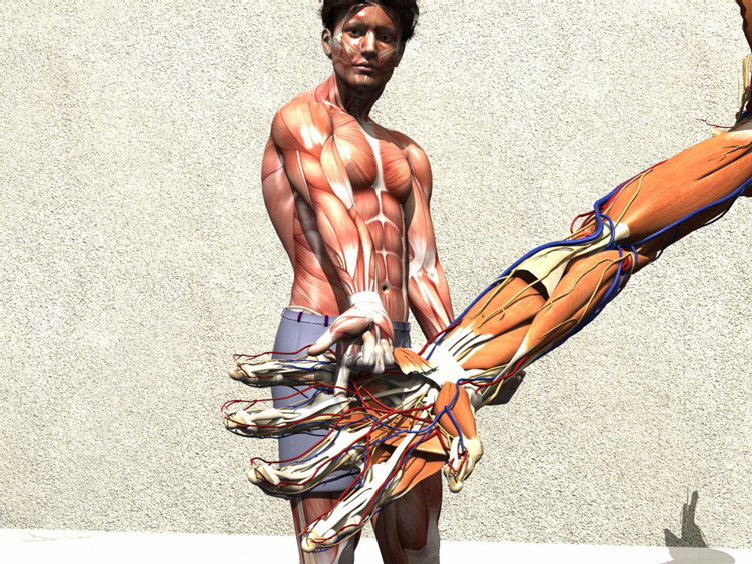
Yank! Yeowwwwww. The kid just ripped the superficialis muscle tendon unit out! That's it on the ground. Notice that the muscle bellies though having a certain amount of unique longitudinal tensioning are more structurally one muscle mass. Lifting this one unit and sliding it distal is a surgical method of generalizing more tendon length to the PIP joints. The nerve must be mobile enough to take the ride for this to work. The kid found another tunnel. He has his pointer finger in the opening deep to the pronator terres under which pass median nerve and some juicy blood vessels. A gung-ho weight lifting binge can swell this muscle and cut off the circulation and the nerve and even present as an emergency.
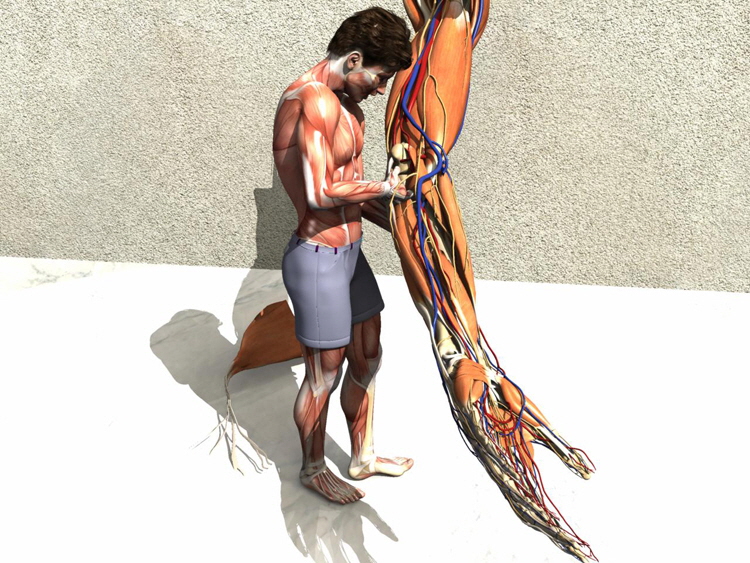
On the back of the elbow, the ulnar nerve passes behind the humerus medial condyle in a groove - the ulnar groove. From there it passes (within a sheath of ligamentous tissue) deep to the flexor carpi ulnaris (FCU). The ulnar nerve runs the length of the forearm applied to the underbelly of the FCU.
This tunnel with the ulnar nerve is apt to bang into things and zapppppppp the nerve - called the funny bone. The funny bone isn't humerus, it is nervous. This canal if tight produces a paralysis of ulnar motors in the forearm such that the 5th and 4th flexors get scar from denervation and contracted curl the 4th & 5th fingers. It is called the BENEDICTION HAND. When the humerus is fractured distally (say a supracondylar fracture or like that), then dense healing tissue in this tunnel may not grow with the tunnel and is a source of ulnar nerve palsy. It may even take ten years to manifest (failure to grow) and thius is named TARDY ULNAR NERVE PALSY. Benediction posture in a hand that is on and arm that once had an elbow fracture needs attention. Nerve loss can be avoided by opening this tunnel. Occasionally - only occasionally and especially if delayed too long - the ulnar nerve has to be moved from the tunnel altogether to be in front of the elbow (under zero tension permanently). Yeah, right. Odd name? But break it down: stenosing (very tight something) and teno (tendon involved) vaginosis (a soft tube has something wrong = osis or inflamed = itis). Tendon stuck in a tight tubular pulley or tube, maybe rubbed raw & inflamed. Many examples around the body including bicipital tendonitis (shoulder) but for this page we have two biggies. Trigger finger or thumb and de Quervain's syndrome.
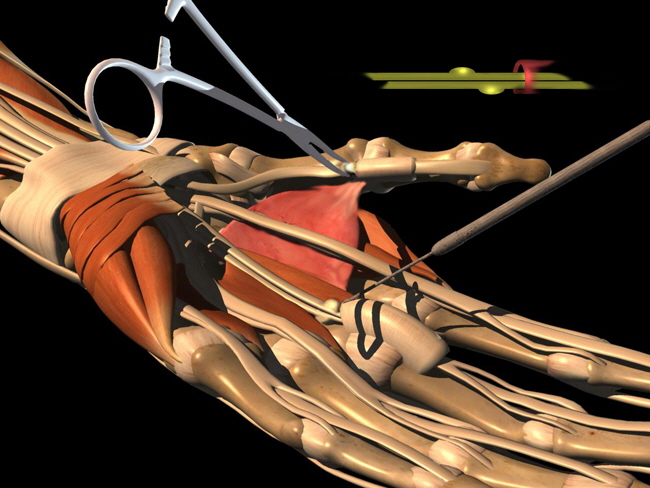
At the base of the thumb, actually wrist level where a watch band would be, the retinaculum band at the wrist passes some tunnels which are pulleys for tendons. The red arrow singles out one in particular very prone to being 'too tight' and making for a very painful use of wrist-thumb combined movement. This deQuervain syndrome isn't totally random as a high percent of cases have an extra tendon (duplicated tendon, and you thought you never got something extra for nothing). There are all sorts of drag it out, inject, stretch and daemonic torture therapies. What works quickly is a snip of the tight sheath - ahhhhhhhhhhhhhhhhhhhhh!
Like a tight hat or a tight collar that chokes you, ointments and things that cool, burn or smell just can't pack the great feeling of getting the pressure off.
The sheaths that the finger and thumb tendons traverse can and occasionally do rub the tendons.
In the case of the fingers two tendons share the swelling and half is in the superficial tendon and half in the deep tendon.
This means that if you bend the base of the finger just so and the tip just so, then the two halves of the pearl swelling can be offset such that the combined swelling outline is smaller and can pass. See the inset drawing above. That is the trick to unsticking the trick trigger finger. Having done that it may pick up some lubrication and then not trigger or 'jam' as much. Of those found in the nursery - some go away. Poof. Some. Most don't or quickly return. The older kids have less odds but with the trick some might self cure. Again most become an annoyance. The definitive fix is shown as making a cut in the sheath. Adults can have this done under local. Kids will never hold still and so get general anesthesia. There is no big deal to waiting. No need to go broke with expensive therapies. They are not going to do more than what the youngster does just playing. But - this is important - if the joint REMAINS stuck for a long time (2 to 3 years) then the unmoving joint growth produces a flattened joint which won't work well even if you do fix the trigger. Also cartilage that receives no opposite cartilage motion deteriorates. OK to wait but not for Hell to freeze over.
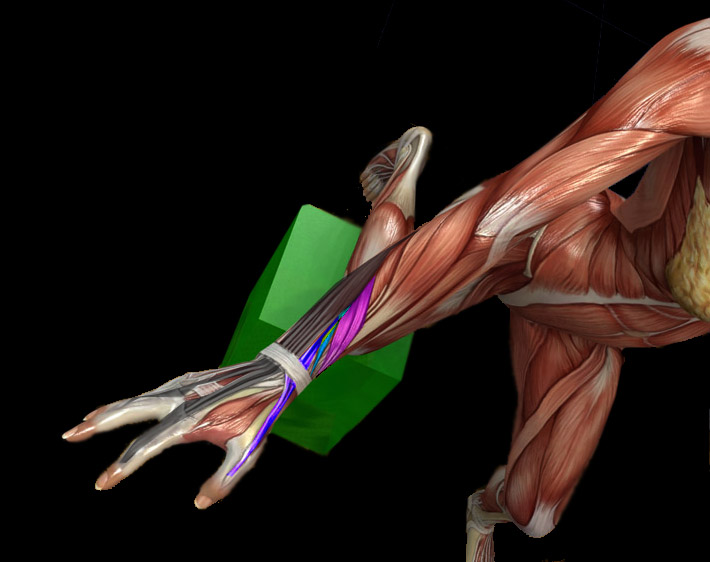
We have artfully avoided talking about finger motion. Why? because it defies talking about. Here we see on the index and middle fingers the hand of the Great Creator. Magnificent. There is a hood into which the extensor tendons weave and terminate. But from the sides, certain intrinsic muscles of the hand (intrinsic = contained totally within the hand) also attach. The interosseus (originating 'between the bones', the metacarpals specifically) sneak up and attach. They can add to extension as well. There are also intrinsics that originate from the long finger flexor tendons! Whoa. Cool. Way cool. And they too, from the palm area sneak up the side to attach to the extensor hood. So the lumbricals modulate finger flexion tension into the extensor tendon mechanism via that hood. But depending on whether the approach of the small muscle tendon slips (we call them slips) pass slightly forward or behind the joint center that action can go from flexing to extending. They can do both. And the hood does slide forward and backward in certain useful movements allowing for outrageous complexity and fine tuning. If this interests you - GET HELP! Take up harmonica, play bridge, anything but this. This takes total dedication and intense study and practice dissection to master. Sorry. But that's the truth.
Here, the lumbricals are shown colorized yellow. We are looking at the palm of the hand with the carpal tunnel partly open. The sublimis tendons are seen directly but the profundus tendons just deep to them are a bit obscured until they zoom out where the sublimis opens at the finger PIP joints (proximal interphalangeal). ['sublimis' = more toward surface, 'profundus' = deeper] The dorsal interosseus intrinsics are between the metacarpal hand bones. The first dorsal interosseus is essentially a direct extension of the flexor carpi radialis in that it begins where the FCR ends and attaches to the extensor hood of the index. You can see it. Hover the pointer over the image parts to see their identity. Remember 'lumbrical thumbrical'. That is the lumbricals kind of mimic the thumb in their course. All go distally and curve toward the ulnar side of the hand as does the thumb. The first two lumbricals take origin from one profundus tendon each. Lumbricals 3 & 4 span the adjacent finger profundus tendons (two profundus tendon origins each). By the way, the first dorsal interosseus does that as well in that some of its origin is from the base of the thumb metacarpal. By attaching to the extensor hood from this position they can still flex the MP [metacarpal phalangeal] joints while extending the PIP joints. The posture of the hand with the finger MP joints flexed 90 degrees but with the rest of the finger segments extended looks like a snake about to strike. It is called the ?snake ready to strike posture???? No. Sorry. It is called the intrinsic positive posture. I warned you. As neurological control of the intrinsics sharply defines median and ulnar nerve function, very subtle postures of the fingers at rest can be read as median or ulnar nerve damage depending on the subtlety. However, sometimes the normal nerves miss a turn off up stream and get there by another route in which case we see exceptions where a fully cut ulnar nerve has no intrinsic loss (in a median dominant hand, the ulnar intrinsics got there by hitching a ride on the median nerve). So this is why hand surgeons like to do specific nerve testing. It isn't that they forgot what goes where but rather that a percentage of people have alternative blue prints.
|
 therno A
therno A







 OK, here's more. You don't give up, do you?
OK, here's more. You don't give up, do you? |
|
 |
||||||||||||||
|
|
||||||||||||||