|
|
||||||||||||||||||||

|
|

 |
Know what holds that medial structure up? highlight[MAGIC]. Yes, has to be, if the tibialis anterior muscle isn't active. Ooooo, wait, no - the tibialis anterior. Yes the anterior tibial muscle holds up the inner foot arch. See also (arch structure) Many kids have a lazy eye kind of flat foot. They have not figured how to turn that muscle on. . . so it droops flat. |

|
Practicing walking on the outer edge of the foot - also called the ice skater exercise - helps jog this muscle into use. It helps discover the T.A. (TA = Tibialis Anterior = Latin for the muscle anterior to the tibia, could have been the shinus infrontof-is). Cups in the heel of the shoe (to better grip the heel) plus a medial wedge will passively hold this droopy foot until the muscle gets awakened or everybody gives up. Watch two sibs - one who has the floppy flat foot when you ask them to walk on the outer edge of the foot. The one with normal arch does it immediately and asks - now what? Meanwhile the other, with the flat foot, is making faces as if trying to tie a cherry stem with his tongue. You might as well have asked him to wiggle his ears. THAT difficulty is the source of flatness is these kids. But there are other causes as well. Beware, tight calf muscles - 'tight Achilles' - also cause the foot to roll toward flat footed. The joint under the talus relieves pressure sideways to prevent the talus from getting crushed. This is not just a flat foot, it is a foot FORCED flat. These are the ones that hurt, that ache, that give shin splints, that give flat feet a bad name. The force is the pain source, not mere flatness. Fixing flatness does not treat the pain. The flatness is a deformation from insufficient calf muscle suppleness. The forces from that cause pain. There are ethnic feet that are simply built flat. No arch by design. They do not hurt and they don't do anything bad unless you try to make them unethnic. Who? Think tropical and great jazz with wonderful complex rhythms. The above movie also shows the path of the tibialis posterior. It runs down behind (posterior) to the tibia and attaches to the navicular bone. This muscle pulls the foot down and under and inward (if far => club foot posture). When this muscle is abnormal and can't grow, it clubs the foot. The spastic tibialis posterior is a beast to control as no brace has a place to hold effectively so as to counter this nasty twist. The TP generally needs to be transferred when it goes bad as the conservative methods fail, fail fast, and are nastier than the surgery and never end.
Duh. No. That's wrong. If it is 11 past the hour and a guy with a gun has a terrified look on his face - don't jump up and yell boo! He will shoot you. It isn't that he shoots at 11 past the hour, it is you yelling boo. So if the muscle is very twitchy and hip flexion is brisk, fliping that leg out, the calf getting a boo from the quick knee extension stretch may very well fire - and yes it IS too soon but not because it is soon but because it is stretched. So the foot suddenly - too soon - points down from that hyper-reflexic REACTION of the calf muscle. Note the bigger spool is the medial femoral condyle and so the medial gastrocnemius is more likely to be spooked into premature action making it hard to clear the ground with the leg with the foot pointing down. You have to lift the ankle quite high to clear a foot pointing down. If there is no contracture (range is full) but this over-reaction is consistent then we can move the attachment of the upper medial gastrocnemius from its position over the condyle to the medial side of the knee (at the base of the medial collateral ligament). Nothing is lengthened nor weakened by this. It is length neutral. But - the 'out of phase' nonsense goes away. Basically the knee extending no longer pulls on that trigger happy bit of anatomy because it is now attached to the neutral axis (center of motion). This trick is called recession , where a muscle with more than one thing to do has one job removed to get rid of its reactive response from the less important job. Also notice that if we were to attach the distal end of the gastrocnemius to the tibia making the usual working moving end fixed and immobile then this end of the gastrocnemius near the knee becomes a pure knee flexor. That is a recession that augments function in an area devoid of it. [actual example]
Here are the main foot pointer-downers (aside from the calf muscles, Achilles & its three muscles removed here). On the far side the peroneus muscles. On our (medial) side the Great toe flexor (great toe = 'hallux'). Just forward that is the flexor to the toes, the flexor digitorum longus to toes 2-5. Forward that (deep to the FDL) is the tibialis posterior. From front to back they are called : Tom, Dick & Harry Tib posterior, Digitorum flexors, Hallux flexor.
The long toe flexors get a boost from shorter muscles in the foot
The peroneal muscles are seen better from the front-lateral oblique perspective. Although they travel downward they use the pully of the fibula to pull the foot laterally and a bit upward - eversion'. That bump on the side of the foot is the base of the 5th metatarsal. The peroneus brevis ends there. The longus dips under to travel under the foot.
The great toe has its own long extensor.. Toes 2-5 share one. Sometimes a unique fifth extensor is also present (the extensor tertius). The tibialis anterior is an upward puller that attaches to the top of the foot on the inner edge. It dorsiflexes and inverts the foot. The common extensor to toes 2-5 is seen with a deeper short muscle covering the midfoot with muscle. The extensor brevis and the extensor digitorum longus have redundant functionality and so muscle transfers have many potential variations possible.
There is very important physics for foot-ankle and knee mechanics in the Torso section. The gist is this, if the foot or ground contour produces a brief upward thrust right before swing phase on the stance leg going into swing, then the hip needs to accommodate that up movement by a passive hip hike on the center of mass (hip to center-of-mass harmonic is about same as the forefoot and the two can cover these inertial variations between them). What? That was too dense? What legs do is try to accommodate the ground while the body floats smoothly forward. That smooth forward travel is dead center body below the belly button. If the leg can't do some bendy thing to accommodate the ground rise then the hip on that side gets pushed up. If the center of mass stays put, then the hip rising on that pushed up side is paired with the opposite hip going DOWN - a sea saw centered on the center of mass. Throwing some attitude into ankle motion REQUIRES the hip on one side to rise and the other to drop if energy is not to be thoroughly wasted. So a fanny wiggling in the quest for ALLURE is NOT the same as 'Trendelenburg' gait in which the center of mass drops along with the swing side hip due to abduction weakness of the support leg.
|
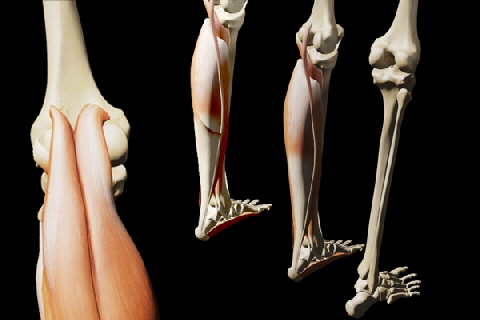 The gastrocnemius muscles attach above
the knee and so they get pulled on when the knee is extending. If the muscles are too sensitive they can fire
The gastrocnemius muscles attach above
the knee and so they get pulled on when the knee is extending. If the muscles are too sensitive they can fire 
 If you take careful inventory there are
close correlates with those muscles found in the hand. Notice that the great toe has a very obvious adductor.
If you take careful inventory there are
close correlates with those muscles found in the hand. Notice that the great toe has a very obvious adductor.
|
|
 |
|||||||||||||||
|
|
|||||||||||||||