Selective Dorsal Rhizotomy
Baclofen
Alcohol
Botox
General Information
Neural
Mechanisms of Spasticity
This section compares items that are often discussed as alternatives. See the buttons for more detailed discussions of each topic.
General Information:
The neural circuits are interesting. There are speed receptors in the muscles. Shaped like spindles, they are called spindle cells. These cells send back a barrage of signals as muscle velocity increases.
The nerves from those muscles end in the spinal cord and end on several nerve cells, called internuncials, whose job is essentially that of an information center. They acquire incoming information and repeat it to other cells in varying combinations depending on yet other information which is coming in before relaying it on to the brain.
Why? Probably reaction time. You see a tennis player doing all ants in the pants movements while waiting for the serve. That movement keeps up a stream of stimulation to many neural circuits via the internuncials. That prepestering lowers the threshold for the actual final response when that ball finally comes. If the player just stood there, cold, then the decision to move would require setting up a train of impulses over the let's-do-it pathway. That train takes time. A single stimulus is all that's needed if the circuit is prepared for action, ready, warmed up, recruited - pick your favorite term.
The internuncials have templates of patterned stimulation to many places and also patterns of inhibition which, together, facilitate action combinations; that is, likely combined movements. The many patterns of movement that can be called upon by the internuncials are under normal circumstances generally inhibited and controlled by higher centers. Failure to inhibit the internuncials releases like a Pandora's box patterns of uncalled for movements and inhibitions. The internuncials not only can make certain pathways more quickly accessible, they can make others inhibited to the point of being inaccessible. A fallout of this is that a muscle that appears to be completely paralyzed may in fact have a connection that is intact but with an inhibition level set so high that it can not be used / recruited.
What if the internuncials get overactive and blast out those patterns of stimulation and inhibition with too little cause? Then certain muscles, even away from the pathway in question, will get recruited and others will defy being activated even with concerted effort.
If the internuncials are given uncontrolled free reign, life gets stereotyped into gross, recognizable patterns of mixed ability and inability. Spasticity is the condition wherein the internuncials are turned up full blast and overreact to incoming information.
The reason is that the internuncials are normally inhibited (made less responsive) by a control pathway from the brain. With that pathway depressed, the internuncials act under their own pre-patterned programing.
The internuncials stimulate each other (talk to each other) with a neurotransmitter called gamma amino buteric acid or GABA
So, nerves don't just fire when stimulated once. They need to be pestered. Like a mom being pestered for candy by the little one. It takes a battery of stimuli (mommy mommy mommy please mommy mommy) from one nerve to make the next nerve in the circuit (mom) respond. That is unless there are additional stimuli on that same receptor nerve from elsewhere (hey lady, give the kid some candy already).
This isn't an all or none process. Some internuncials may be behaving fine (maybe they still have brain connections intact) while others are totally out of control.
So what can you do to stop this? Well you could determine which nerves coming into the spinal cord carrying information lead to barrages of motor activity going out. In theory, sensory information coming in ought to facilitate voluntary moves but NOT initiate moves of their own. If you stimulate a sensory nerve under anesthesia, nothing should happen. The motor nerves should be quiet, as under anesthesia the brain (not the spinal cord) is asleep.
But if a sensory stimulus is followed by a blast of motor activity over a bunch of motor nerves, then that sensory nerve is connected to a nasty internuncial, one that acts alone. Since we can't get at the internuncial cell itself (deep in the spinal cord), we can cut the nerve fiber that connects to it, thus turning it off.
 |
Selective Dorsal Rhizotomy
"SDR"
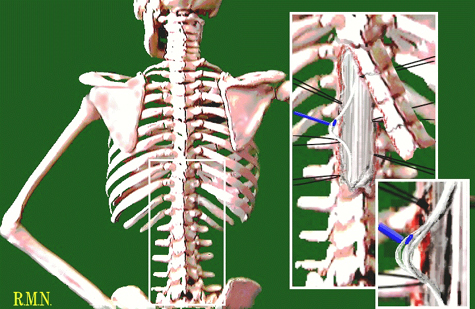
Dorsal means backside. Rhizotomy means cutting nerves. The spinal cord has some nerves coming out the front and others coming out the backside. The backside (dorsal) nerves are all sensory nerves. Selective means that only certain sensory nerves are cut while others are left alone.
Why cut some sensory nerves? Spasticity. Spasticity occurs when the control over spinal reflexes is so altered as to allow returning sensory information, coming from muscles, to incorrectly loop, in the spinal cord, into outgoing motor circuits. That is, muscle sensory information echoes back to the same muscle in the form of motor nerve activity. This tells the muscle to act again. This is a vicious cycle. This loop may also be feeding other muscles to act by way of the internuncial which has many connections to other circuits.
So we need to stop the looping recycling stimuli. Cutting the pathway on the motor side would not allow normal motor commands to be sent to muscle. Not good. Not done. Cutting the loop on the sensory side gets the job done without losing the route for normal output to the muscles.
In the picture, above, you see the back of the spine. The enlarged inset picture shows the unroofing of the spinal canal exposing the spinal cord and the nerves coming from the cord. The nerves on the surface are sensory nerves. The motor nerves are on the deep side and are not seen here. The second detail inset picture shows subdivision of a nerve into sub portions. These are electrically stimulated one by one. There are many many many sub nerve fibers. One by one they get stimulated by the neurosurgeon as the physiologist reads the electrical waves on the muscle probes. The physiologist may report back "Quiet." in which case the next one gets tested. Or, "That one is making three muscles go wild." Actually it is much more boring technical talk but that is what is being conveyed. Wild? Cut that root. Get rid of it . Why? It isn't doing good. It is doing bad. Won't miss it.
Recap:
Normally, muscles in the leg should remain quiet as sensory nerve stimulation is performed. If there is significant activity in leg muscles when such a sensory nerve portion is stimulated, then the sensory information from that path must be 'leaking' into motor pathways (this leak takes place in the spinal cord internuncials). If such leakage is found, then this sensory nerve segment is cut.
A limit is placed on the total percentage of nerve rootlets that is allowed to be cut, regardless of the findings, as some sensory input is vital to function as well. Other aspects of neurologic injury (rigidity, floppiness, athetosis, learning or perceptual disorders, balance mechanism deficits, motor planning etc.) are NOT treated by rhizotomy.
Rhizotomy is NOT a treatment for cerebral palsy. It is a treatment for feedback on the velocity reflex loop. That feed back is seen clinically as "spasticity". Spasticity is NOT stiffness. It is over-reaction to quick moves. Stiffness in muscles may come from elsewhere in the nervous system. We use different names for the different flavors. Rigidity is one kind. Dystonia is another kind. ... Only spasticity is treated by SDR.
We already noted that internuncials stimulate each other and other nerve cells. They do so with the chemical called GABA. If you take the GABA molecule and put a small extra chemical thingy on it, you get a false GABA that binds to the transmission sites without stimulating. In fact, it blocks transmission. This false GABA is called Baclofen (oral version = Liorisal).
A drug called Baclofen blocks the chemical neurotransmitter that is involved in this spinal neurologic cycle. Baclofen can be used for a purpose similar to rhizotomy.
If given orally, it takes a lot to get it into the spinal fluid and deep into the spinal cord so as to tone down the internuncial cells. So you give a lot. The problem is that the brain also uses GABA as a transmitter. It is just a matter of luck. In some folks the brain barrier to Lioresal or Baclofen (same stuff) may be good enough to make spinal treatment easy. In other folks the Baclofen or Lioresal gets to the brain sites with as much ease as to the spinal cord. If so, we see the brain side effects... behavioral goofyness, etc. There may even be seizure related interactions.
One advantage of Baclofen, is that its action stops when it is discontinued. It therefore is especially useful in neurologic injury in the early stages when the severity of spasticity is at its worst and is expected to gradually lessen. Baclofen can be tapered as need indicates.
T o avoid brain effects it can be delivered directly to the spinal fluid, using a pump, delivering
as much as 1000 times the dose as seen by the spinal internuncials, with no brain side effects.
o avoid brain effects it can be delivered directly to the spinal fluid, using a pump, delivering
as much as 1000 times the dose as seen by the spinal internuncials, with no brain side effects.
This is the pump. There are two sizes, big and huge. The "pediatric" one is the big one. This is a picture of the huge one. It is a hockey puck.
It is not an easy drug to control, however. Long term Baclofen treatment involves implanting an internal reservoir and pump to bathe 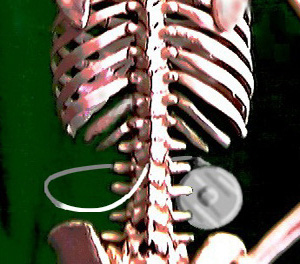 the spinal cord via a tubing threaded into the spinal canal as seen on the right.
the spinal cord via a tubing threaded into the spinal canal as seen on the right.
As you can see above, the pump size is an issue. Add to this, VP shunt tubing and a G-tube and golly how do you brace this if scoliosis occurs? By the
way, that's 50% of cases wherein scoliosis occurs. It isn't easy. But see the scoliosis discussion on special CP bracing in the scoliosis treatment  section.
section.
In some very impaired patients, when mental capacity is not an issue, an oral version of Baclofen, called Lioresal, can be used and given in higher and higher doses, as an oral medication. Long term effects of this treatment are not documented as of yet. Typically it is used, in difficult circumstances, to get through some immediate need.
The inherent problems of difficulty of controlling dose, and of growth  disturbing the implanted plumbing, limit Baclofen pump implant treatment to the older population. As a generality, Baclofen is used in the adult patients, typically with
adult onset neurologic problems, and selective dorsal rhizotomy is used in young children with predominantly spastic (not rigidity) problems.
disturbing the implanted plumbing, limit Baclofen pump implant treatment to the older population. As a generality, Baclofen is used in the adult patients, typically with
adult onset neurologic problems, and selective dorsal rhizotomy is used in young children with predominantly spastic (not rigidity) problems.
Interestingly, Baclofen seems to have some efficacy in rigidity whereas SDR does not.
Remember, spastic muscle activity is only a part of the disorder associated with either cerebral palsy or stroke. When the spastic component is the limiting and most damaging component, then either of these two treatment forms may be considered from a list of various alternatives.
When spasticity is focused on a single muscle group or narrow category of function, more local or directly oriented (muscle procedures etc.) make more sense. When contracture (actual loss of the range of motion of the joint) has become prominent, specific mechanical repair of that limitation is a good idea even if more broad spasticity remedies, such as rhizotomy, are used.
We have been surprised to find that reduction of spasticity via rhizotomy does NOT necessarily prevent muscle contracture (fixed structural shortening) with growth. Clearly some other factor is at work here. Nevertheless, such contracture, if it occurs, can be remedied by muscle specific lengthening procedures and need not become a limiting factor in functional progress. The key issue is that fixed contracture can mimic a "wearing off" of rhizotomy. In fact, in nearly every single incidence of supposed rhizotomy late failure, muscle contracture is at fault. The rhizotomy can be rejuvinated, so to speak, by dealing with the muscle lengths.
LOW DOSE BACLOFEN
Baclofen has gotten a bit of a bad rap due to the number, or more correctly, percentages
of kids who can't take it due to baclofen complications. The most common problem is getting gooney and unable to process information. The numbers are so high as to
suspect that the treatment protocol may be partially to blame.
We have found that problems are far fewer IF
much smaller dosages are used
and
the dosage is built up very slowly with an eye to quitting when a very specific end point is attained.
So pick a desired result (cure of CP isn't one). Something like being able to let go of a
grip or being able to sit all the way in the chair, or not always have the one arm behind the back.
Then begin at 1 (one) milligram taken nightly (only) and held at that for a week before
going further into dosage. Some of the Baclofen effects evolve rather than bang into being. Give it time. Then add 1 mg each week by either adding it in AM then in PM
alternately or by weighting the daytime the effects are most desired.
The pharmacist is brought in to prepare a solution that allows this as currently the lowest dose is 10 mg which is too much for many of our kids.
This isn't a panacea but does allow some kids benefit who have no other better options.
Generally avoid Baclofen when seizures are prominent. Only do this with the oversight of a local physician (neurologist or physiatrist etc). Also the pump is aimed at having
very low dose systemic exposure while having effective levels where it matters.
Even so, having a realistic and limited outcome goal makes a huge difference. Otherwise
dosages escalate until an undesired effect happens. That guarantees bad statistics.
Another more detailed Baclofen discussion digs into the deep bits.
What has alcohol got to do with internuncials? Nothing directly. But indirectly, much. Alcohol (booze, ethyl, not talking about the alcoholic chemical called phenol), when injected right on a myelinated nerve strips the fat away. It creates a bald spot in the myelin. Myelinated nerves transmit impulses much faster than unmyelinated nerves. But the bald spot acts like a speed bump in the nerve. Fast trains of impulses pile up.
So when a fast train of stimuli from receptors hits the speed bump, the internuncials don't receive "mommymommymommymommymommy" but more like "ahem, mother...................... if I may, mother.............". Thus the internuncials don't get the rapid fire background stimulus that pushes them over the edge into stimulating their neighbors and every other nerve on the block.
But alcohol, used in too large a volume can cause a burning sensation if it gets to mixed nerves. You need to have the capability of exactly placing a needle directly on the target nerve so as to inject a small volume of alcohol that won't spread too far.
For that, you need special needles attached to special electronic 'nerve finder" circuitry. The sparky needle procedure isn't comfortable, so, it is usually done under anesthesia.
Alcohol blocks in babies last from six months to three years. It isn't the alcohol that "lasts", but the repair rate of the child in fixing the speed bump caused by the alcohol. Often there is some residual long effect. Used in older children it lasts longer as the ability to repair alcohol 'damage' gets less. In a 10 year old a single block should last many years, maybe even functionally permanent as the circuits adapt.
The most common alcohol block is to the obturator nerves. That circuit has significant effect
on the cross stimulation between adductors and hamstrings - big players whose cross reaction feedback bleeds in to many other circuits. We can get rhizotomy like effects in very young
babies, allowing them do do stuff that otherwise is muddled by all the internuncial shenanigans.
More on alcohol and phenol blocks
Where nerves touch muscle, the spot where nerve activates muscle, is a mechanism of communication. When the nerve wants the muscle to act it says " Go!" but in the language of chemistry. It releases a go-chemical called acetylcholine. Botulinum toxin is a gag on the nerve such that the nerve says "mmmmffff mmmmfff" or just "". Without a "go" the muscle waits.
However, we are certain - in our practice - that a second unmentioned Botox effect of greater importance is that same action on a very specialized structure within the muscle called the "spindle". The spindle is a velocity/acceleration receptor (whose nerve feedback is what feeds the spastic loop). The spindle is made of two forms of muscle. We are certain, because of contralateral (opposite side) effects that the spindle is the primary active site for the Botox, more so than muscle in general in spasticity. This is a theory, our theory. We'll see. Could be wrong.
Additional information on Botox is found in Paraspinal Botox and on the manufacturer's site for general information, intracell targets, and mechanism of action and a dedicated section Botox.


