|
Elastic Simulation of Spasticity
An interesting experiment which may change the way you think about spasticity.
It is very interesting to discuss the failures in implementing this study. In fact, the most important information resides in how this study required three
attempts. It was a simple idea. We had already engineered devices to be worn by normal volunteers which restricted one joint or another by such and such an amount. Then we measured walking to see what effect limited
range had. We were interested in the devices limitation itself but more so in the way things behaved which were NOT constrained. In other words - how does a free ankle compensate when a knee has half of its arc of
motion blocked? Compensation.
Very interesting was the movement of a totally free leg opposite to the leg we impaired. Subjects were paid to just keep walking (all day long) as the
impairment was modified and the walking results remeasured. An endless stack of hot pizzas and bottomless colas and fruit were eaten on the fly (while walking). In no case did any subject belly ache about what was
going on. They knew in advance that it was a full day of walking. These experiments, in various forms were of joint RANGE but the joints were free and unfettered within those narrowed ranges. That is, there was no
graduated resistance, just metal stops.
With full passive range available the elastics were set to stepwise constrain combined
active range of hip&knee. The full range was that tested without elastics setting the norm for that subject.
This study, the one that twice failed, was just the opposite. It was set up to see what
would happen if joints were free through a full range but resisted by elastics of various strength. Why did it fail?
The first subject, a young adult jogger quit halfway through when he could no longer get
his breath and was panting fiercely face down on the floor. He had resorted to crawling to get to the place to remove his torture implements. He had, in his last trials before quitting,
dived to cross the infrared beam rather than stride across.
The next subject was a marathoner. He made it 3/4 through the planned series and then
went the way of the first subject. He too crawled in the quest for relief. It was just as well. The EMG telemetry had also failed in both cases. On the first pass the signal went off
scale beyond our ability to dial the gain down to a range that could be read. Our sure fire potentiometer remedy did not do enough in the second study either.
The third pass went logarithmic both electrically and subject wise. We found a 9 year old
international competitive Irish step dancer - someone apparently incapable of fatigue. We paid a substantial sum of money for time walking and threatened a penalty if it were to
cease. We put our circuitry for EMG in line with another labs such that we could achieve a 1000 fold signal reduction in gain.
Twelve trials were performed. Two were without anything at all testing the pressure
measuring foot pads and making sure they did not affect the walk. They didn't. We tested the garb. That was a rubberized nylon body suit glued on with medical adhesive and shin
"socks" of the same stuff glued on the shins. The walk was the same as no joints were impeded by these garments. The garments were so constructed to anchor both ends of
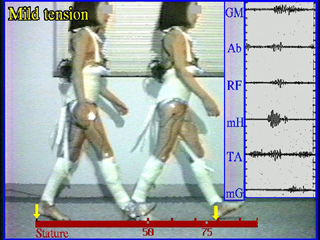
what was essentially a semitendinosus in the form of an elastic. We tested three levels of mild, then moderate, then severe elastic resistance.
Mild meant that the patient could flex the hip 90 degrees and actively fully extend the knee.
Moderate meant that the knee could be actively extended if the hip were flexed 70 degrees
. Severe meant that the knee could only extend with effort if the hip were extended at zero.
That is, there were nine levels of resist and the tenth was garbed with elastics removed
(same as control but after the others were completed). We called this "post-op".
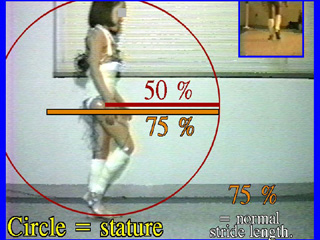  Garbed without elastics. That is free walk. The measure used by us is not feet or meters
but rather "statures". A stature = height. If a full cycle thing is being measured then a travel equal to 75% of her height is a 75% stature travel. By the way, statures make life
easy. Normal gait is 75% stature regardless of age. You can lost those tables. Also, the data fits far tighter as it isn't against pooled data tables. Garbed without elastics. That is free walk. The measure used by us is not feet or meters
but rather "statures". A stature = height. If a full cycle thing is being measured then a travel equal to 75% of her height is a 75% stature travel. By the way, statures make life
easy. Normal gait is 75% stature regardless of age. You can lost those tables. Also, the data fits far tighter as it isn't against pooled data tables.
When we measure a half cycle thing (a right step, for instance), then we use the radius
(1/2 stature) as our measure and call that a stature as well. So a travel over a single leg step is also 75% stature. A very robust assertive stride may tickle 80% stature and a
tentative stride may drop to 70% ish.
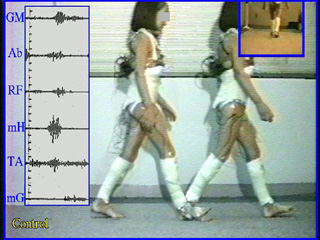 EMG is the measured electrical activity emanating from a muscle. It is like a cardiogram except that the muscle of interest isn't the heart. Sensors are placed
over selected muscles. As muscles recruit more and more sub-elements the size of the tracing gets taller (voltage). But muscle works hardest by staying active longer and
longer. On the left we see that for any given muscle, it is mostly quiet until a brief oomph of activity timed to its BRIEF contribution
to walking. Thing of yourself pushing a kid on a swing. You do little most of the time, then briefly give a small push to maintain the swing. Conservation of energy in gait utilizes EMG is the measured electrical activity emanating from a muscle. It is like a cardiogram except that the muscle of interest isn't the heart. Sensors are placed
over selected muscles. As muscles recruit more and more sub-elements the size of the tracing gets taller (voltage). But muscle works hardest by staying active longer and
longer. On the left we see that for any given muscle, it is mostly quiet until a brief oomph of activity timed to its BRIEF contribution
to walking. Thing of yourself pushing a kid on a swing. You do little most of the time, then briefly give a small push to maintain the swing. Conservation of energy in gait utilizes 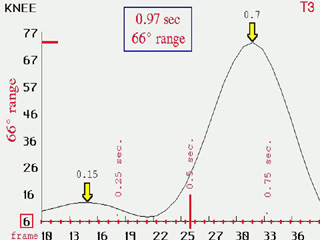 pendulum action. It is the same. If the leg
pendulum is dampened (if the kid on the swing gets stopped by somebody else) then the momentum must be restored anew (bigger oomph) before small timed short bursts will be sufficient again. The Tibialis
anterior line is a bit noisy as it really picks up several adjacent muscles. pendulum action. It is the same. If the leg
pendulum is dampened (if the kid on the swing gets stopped by somebody else) then the momentum must be restored anew (bigger oomph) before small timed short bursts will be sufficient again. The Tibialis
anterior line is a bit noisy as it really picks up several adjacent muscles.
We see that this youngster is using about 66 degrees of range of motion of the knee in swing phase and about 10 degrees in stance on
a flexion baseline of 6 degrees. Timing and event maxima are also noted. Other joints are also measured.
 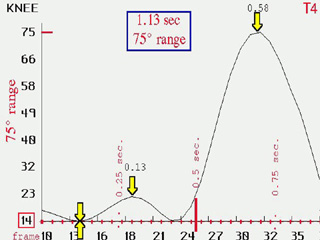
The milder elastics seem to make no difference at all. This is normal gait, but then, notice
that the baseline of flexion is greater. Essentially, given a gentle resist, the youngster just flexed enough (14 degrees) to make the resist go away, then from that, walked normally.
You would hardly notice it in the EMG.
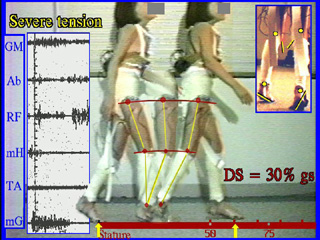 By the time we get to the more severe elastic settings, the patient has been long walking on her toes. Toe walking began in the moderate range and persisted through
the remainder. She began to plead for rests. Sorry, no rests other than to change the elastics. By the time we get to the more severe elastic settings, the patient has been long walking on her toes. Toe walking began in the moderate range and persisted through
the remainder. She began to plead for rests. Sorry, no rests other than to change the elastics.
The voltage in the EMG was off the scale by moderate and required turning the gain down until by this point the entire range of
gain dampening was used. That is, the EMG would be a wall of black. Here we see the readings at 1/1000 setting. All muscles are just
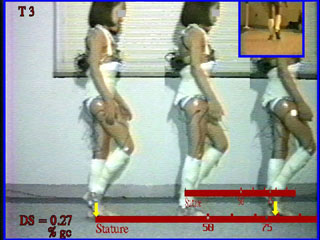
about continually on.. Notice that her knee hardly flexes and extends at all (the stick figures at three points can be superimposed. Stride has become 65% stature. There is inward rotation crouch.
Let's go back to look at the moderate setting in another way to try to make sense of this.
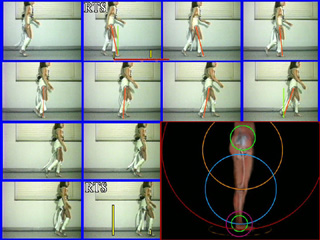 From right toe strike (right foot first touches floor) to the next right toe strike we see that the hip to toe line relative to the hip-knee
-ankle-toe joint positions hardly alters at all. The contributions of motion from each link (thigh, shin, forefoot etc) are consumed by a replacement and much longer combo (the
large red circle). So rather than use multiple circles in a clever way over a long stride, a short stride with a very long circle is substituted. Big circle - small arc. That
solves vaulting and makes motion tangential to the resisting elastic. The toe raise is needed to center the body in this narrow arc - phase shift in engineering terms. From right toe strike (right foot first touches floor) to the next right toe strike we see that the hip to toe line relative to the hip-knee
-ankle-toe joint positions hardly alters at all. The contributions of motion from each link (thigh, shin, forefoot etc) are consumed by a replacement and much longer combo (the
large red circle). So rather than use multiple circles in a clever way over a long stride, a short stride with a very long circle is substituted. Big circle - small arc. That
solves vaulting and makes motion tangential to the resisting elastic. The toe raise is needed to center the body in this narrow arc - phase shift in engineering terms.
Indeed, what knee flexion that is seen on graphs does not happen during anything that
propels. It happens during a rest segment of swing to relieve the tension and let blood flow. The knee flexion is very misleading if not correlated to the actual events.
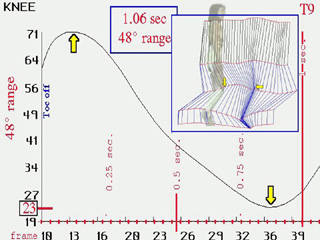 OK, back to the severe case. What we see on the left is a 23 degree baseline plus 48 degrees of knee flexion from that. Nearly all
of it is in swing phase after the hip to ankle line passes vertical. It is "ahhhhhh flexion", relief, not propulsion. OK, back to the severe case. What we see on the left is a 23 degree baseline plus 48 degrees of knee flexion from that. Nearly all
of it is in swing phase after the hip to ankle line passes vertical. It is "ahhhhhh flexion", relief, not propulsion.
Thus we see that the curve on the left is not normal gait reduced incrementally by incremental resistance, but something new.
Something contrived. The solution to the pathology was to use a big circle in small arcs so as to minimize force directly against the elastic restraint. A compromise of effort
from crouch and need to crouch to lessen elastic force is arrived at. The solution to use a stiff longer circle made up of otherwise supple parts requires that all those smaller circles
be welded into one - cocontraction.
 The energy cost was so high that athletic adults were not capable of it. The energy cost was so high that athletic adults were not capable of it.
Thus hamstrings which have an artificial additional (elastic strap) hamstring added on, oddly increase their activity rather than
decrease to offset the experimental addition. This cocontraction may be a hard wired solution - a "plan B", so to speak. Discrete drop in hams may not be a neurologic option even for a world class Irish step
dancer.
Observe how stiff the swing leg is. Motion occurs AFTER stance and BEFORE effective swing. That is, it merely relaxes tension to let muscles recharge. It is not either
propulsive nor for clearance in swing. The graphs of arc of motion can be very misleading if the motion is not keyed to the events (what is functionally going on). Also note toe
walking. [RTS = right toe strike. This is one cycle RTS to RTS.] Clearance comes from 3 places: 1) more stance knee extension at mid stance (when flexion normally occurs) 2) more stance foot plantar action
and 3) sway to stance side holding stance hip stiffly. Very little comes from more swing leg flexion (which normally provides most clearance) even though there is an "excess" of
knee flexor tone in the form of strong elastics. Quadriceps activity is very high and very abnormal looking. Yet this is a better than normal individual. The cost of bending the knee
is having to extend it again at a difficult point in time. The quadriceps excess is a solution, not a problem. The knee extension seen at midstance is akin to what we all do when we
are in a forward momentum conserving strategy - ie, when stair climbing. So normally eccentric motions swap to concentric => "concentric gait" or we like our own term "stair
climbing" gait. Stair climbing is gait robbed of momentum.
Interestingly the maximum knee flexion seen was NOT related to movement. It was the
flexing of the knee to relieve tension to stop cramps. Muscle does not flow well in the muscle while contraction but does so in the longer (normally) rest periods. If you did not
correlate this motion to the actual event (video) then you might err in thinking that there was actually a range of motion 'in walking' when in fact the legs, though crouched' moved quite stiffly.
So then, we pose this question:.
When this 6 year old with spastic diplegia who required full arm support to even be measured walking and who fatigued badly in
mere minutes, with a wall of EMG activity over his lateral and medial hamstrings had only his semitendinosus lengthened, why did the EMG normalize over all those muscles which received no operation?
We assert the answer is in the above experiment.
Another lesson, when SD rhizotomy does wonderfully then inexplicably later fails (the
assumption that the neurologic whatchamacallit reverted again), the answer is in simple contracture. Rhizotomy does >> NOT << prevent fibrous contracture from happening.
When they do happen, the passive elastic force of that contracture produces something that looks a whole bunch like cocontraction and is mistakenly read as resumed spasticity.
Likewise, SD rhizotomy will fail to achieve its one really great effect (supple undampened swing) if baseline fixed contractures are not removed
at the same time.
Oh, and by the way, it does not matter nearly so much that "heels are down" but rather
that brutal energy loss - enough to level strong men - is avoided.
|

