
|
|||
|
|
|
|
|
Offsetting Hand and Upper Limb Problems Abram E. Kirschenbaum, MD
|
|
|
|
|
|
Upper extremity involvement in cerebral palsy interferes with optimal use of the hands. Contractures of the elbows, for example, may interfere with the ability to position the hands in space. Mild to moderate wrist contractures may interfere with grasp and release and limit use of the affected hand as an assisting hand. Severe wrist contractures may interfere with dressing as a stiff flexed wrist is hard to get through a shirt or coat sleeve. Surgical treatment can improve upper extremity function in cerebral palsy. Releases of contracture and tendon transfer are the most common types of procedures. With these techniques it is often possible to transform a muscle that is acting as a deforming force and reposition it so as to have it assist a more desirable position of the involved joint. For example, in cerebral palsy, certain muscles which flex the wrist are often over active whereas other muscles that extend the wrist are correspondingly weak. Moving a wrist flexor muscle with its tendon - and attaching it to a wrist extending tendon - alters the action and promotes a more functional position of the wrist.
Tendon transfers can be used to assist holding that thumb posture so that the deformity will not recur. In certain badly destabilized thumbs (from long standing over extension of the mid thumb) fusion of one thumb joint of the is occasionally necessary to prevent recurrence and to not waste thumb pinch power through an unstable segment.
Swan neck deformities of the fingers are also common in cerebral palsy.
Nonoperative care consists of using 'ring' splints and is appropriate for mild cases. When the fingers actually lock in a hyper-extended position, preventing them from
flexing into the palm, surgical treatment may be helpful. The goal is to prevent the hyper-extended swan neck posture while preserving as much useful flexion range as possible. The hand illustrated is that of a 17 year old male high school senior who has cerebral palsy involving the right upper and lower extremities. Notice the marked flexion deviation of the wrist which is also skewed toward the side (same side as the small finger). There are both thumb-in-palm and swan neck deformities. Neither hand posture nor function was improved with non operative care. He, therefore, elected two separate surgical procedures.
In some cases, improved wrist function can also improve swan neck deformities. In this case, swan neck The following fall, this young fellow went to college the with a greatly improved left hand. He was, in his own estimation, much less self-conscious about his appearance because of the elimination of a fixed contorted posture. At long term follow up the gains made at surgery have been preserved and there has been no recurrence of the preoperative problems. Use of the hand in functional activities is increased. |
|
|
|||
|
|
|||
 Finger and thumb manifestations of cerebral palsy also commonly interfere with daily activities.
Finger and thumb manifestations of cerebral palsy also commonly interfere with daily activities.  contracted muscles in the hand, the thumb can be passively placed in a more open functional position.
contracted muscles in the hand, the thumb can be passively placed in a more open functional position.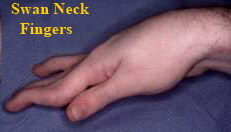
 At the first, a tendon that normally pulls the
wrist toward the small finger was divided surgically and was transferred (reattached) to a tendon that normally deviates the wrist toward the thumb. The immediate post operative photo already shows a
more functional position of the wrist at rest.
At the first, a tendon that normally pulls the
wrist toward the small finger was divided surgically and was transferred (reattached) to a tendon that normally deviates the wrist toward the thumb. The immediate post operative photo already shows a
more functional position of the wrist at rest.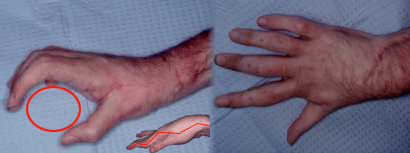 deformities were unimproved and were addressed six months later. A tendon altering operation was performed on each
finger such that half of the tendon that would normally flexe the hyperextended joint is repositioned and tightened such that there is an extension stop point.
deformities were unimproved and were addressed six months later. A tendon altering operation was performed on each
finger such that half of the tendon that would normally flexe the hyperextended joint is repositioned and tightened such that there is an extension stop point.