|
Psoas Muscle Lengthening
Iliopsoas
The hip joint has two main parts. The ball and the socket. The ball
rotates within the pelvic hip socket. The ball of the hip is also called the "head" or cap of the femur
(femur = thigh bone). the "head" or cap of the femur
(femur = thigh bone).
The head of the femur is supported by the angled "neck" which joins to the long vertical body of the femur (thigh bone). At the base of the femoral neck is a boney protrusion.
There are two very large muscles which converge into a single attachment to this protrusion.
The iliacus muscle (which covers the pelvic bone on the inside surface of the pelvis) and the psoas muscle (which embraces the side of the lumbar spine), both attach as if they were one muscle with a common tendon onto that protuberance at the base of the femoral neck. These muscles
do two things: 1) if the leg is allowed to move, the hip is flexed and the leg is raised or swung forward. 2) or if the legs are stabilized, the body sits up from lying down or
stays upright. These muscles are needed for both walking and sitting.
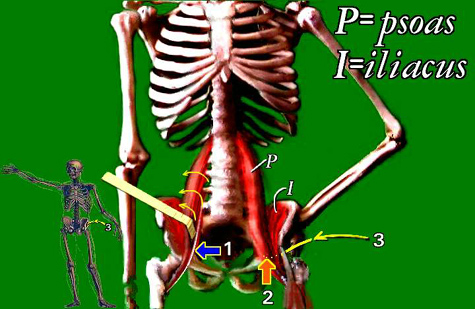 |
The psoas tendon (1) is underneath the psoas muscle (2). A path to the psoas tendon (3)
dives beneath the muscle up into the pelvis.
If both muscles are detached from the femur, then significant power for walking, stairs, and also for sitting erect is compromised. However, contracture from this muscle group
is the most dogged cause of hip subluxation (partly off-center femoral head). Therefore, ways to elongate the muscle without "letting it fly" are practiced. That means getting
at the muscle higher up than the easy spot in the upper leg.
Iliopsoas (or often called just 'psoas') lengthening is performed for a variety of reasons.
The most common, in handicapped persons, is to deal with a dislocating hip. In that setting the hip dislocates because the hip socket is too shallow and too vertical
(reshaped so the socket faces more out, less down) and under severe muscle forces, the strongest being the iliopsoas pair. Abnormal shearing forces of the iliopsoas and
adductors (and others) can cause abnormal growth and shape of the both the hip socket and the upper femur.
The psoas and the iliacus both skirt the abdominal cavity. To get at these muscles,
surgery to reduce ongoing hip destruction associated with overactive iliopsoas tension is commonly directed around the periphery of the lower abdomen on the inside bowl of the pelvis.
This intra-abdominal nature, particularly in the neurologically handicapped, can elicit an intestinal shutdown called "ileus". Ileus lasts from minutes to several days. It is
impossible to predict. It requires feeding by intravenous route while the intestinal protective reflex subsides. The deep nature of the surgery, near the bladder and in the
pelvic floor, requires post-op pain management and, in spastic individuals, antispasm medication. Early mobilization is attempted to avoid adhesions, prior to hospital discharge.
In most cases additional muscle surgeries, such as lengthening of adductors etc. are
done to deal with other paralytic imbalances. These additional lengthenings only complicate the care if they introduce the opposite limb in cases where iliopsoas lengthening is one sided.
Because the psoas muscle is totally covered by intestines and other organs, it is not
accessible to injection from the front. It can be injected from the back, however with x-ray and electrical probe guidance. The psoas is a paraspinal muscle (muscle alongside
the spine), and therefore can contribute to spastic scoliosis in the lumbar area.
Illustration Key: Psoas muscle from the spine, joins with Iliacus muscle from the iliac (pelvis wall) to form the common Iliopsoas muscle. It has a very thick tendon on
its deep surface (slightly inside the muscle). 1) psoas tendon deep to muscle (turned over here); 2)
psoas as it crosses pubis 3) surgical path over rectus femoris and deep to Iliopsoas into the pelvis seeking the deep tendon.
|
