Foot Interventions for Severe Problems
Club Foot
Paralytic Valgus Foot
Macrodactyly
Ectromelia
Deformations: In utero, the feet can be pressed into odd postures. The key thing about such deformation by outer pressure is that the
feet themselves are passive in the process.
In utero, the feet can be pressed into odd postures. The key thing about such deformation by outer pressure is that the
feet themselves are passive in the process.
They would not be that way of their own growth programming. Once straightened out by their own resilience or with a helping nudge
or two (exercises, casts, or shaped shoes etc.), such feet will do fine. They maintain correction naturally, as correct form is already inherent in the tissue blue print.
There are a variety of conservative "corrections". They share a common property, they are gentle
forces applied to the foot in the direction of return of shape. A hands-on manipulation is an externally applied force. A corrective shoe is an externally applied force. A cast is an externally
applied force. The big difference is how long applied and how meticulously shaped. Frankly, many orthopedists cringe at the "exercises" that parents do to their own children in the quest to avoid "braces" (the little white shoe
with the thingy on the bottom). "Exercise" sounds like a nice upbeat word, but it is not rare to see feet literally dislocated by inexpert hands.
Club Foot: Club foot is not just a bent foot. If you straighten a club foot and then let it alone it goes back to being clubbed. That is the one single most important fact about club foot from which nearly every decision can be properly deduced. Club feet
work from a bent blue print. They seek club-ness with growth. Correction of shape must not be merely attained. It must be actively maintained. To not maintain a corrected
club foot is to play Russian Roulette with half the chambers loaded.
Club foot is not just a bent foot. If you straighten a club foot and then let it alone it goes back to being clubbed. That is the one single most important fact about club foot from which nearly every decision can be properly deduced. Club feet
work from a bent blue print. They seek club-ness with growth. Correction of shape must not be merely attained. It must be actively maintained. To not maintain a corrected
club foot is to play Russian Roulette with half the chambers loaded.
Attaining correction of club foot deformity was anything but easy even as recently as the 1930's. In fact adults with
uncorrected club feet sought treatment by prosthetics.
This man had the typical club foot deformity that we see in the new born, except that as an adult he has to walk on it -
as there was no effective treatment for him as a child nor did a late reconstructive procedure exist for him as an adult.
Note the left (club foot) heel at the red arrow and the right
normal heel at the yellow arrow. The orthotist created a raised right shoe with a laced sock to allow needed space to place a false foot below the left club foot, assisted by a bit
of left hip hiking. This was life in the 20's and 30's. Even in the 50's, we saw such folks who had adjusted to this state of affairs.
 |
 How far will people go? In the old days, the options were stark, sobering. It isn't vanity
that leads to a woman seeking amputation and prosthetic substitution. That was the best way to get the best prosthesis for function and least notice from others. It wasn't about getting noticed but rather about not getting
noticed. That is the essential difference between "cosmetic" and reconstructive surgery.
How far will people go? In the old days, the options were stark, sobering. It isn't vanity
that leads to a woman seeking amputation and prosthetic substitution. That was the best way to get the best prosthesis for function and least notice from others. It wasn't about getting noticed but rather about not getting
noticed. That is the essential difference between "cosmetic" and reconstructive surgery.The single greatest problem and the fear of parents was and still is ostracism. Back then, women were apt to select ablative surgery to permit better prosthetics with less risk of ostracism. Such prosthetics were capable of near normal levels of function (see SACH).
What else do we learn from the past? Children and adults with club feet who do not have additional impairments can walk. However, unprotected, the feet take a beating, they become sore, and the gait is unsteady.
But this was palliation, not correction. Orthopedics attacked from two directions: 1) Early manipulative techniques combined with casts and 2) More aggressive surgeries, many of which were made more effective by cast pretreatment. Various surgical strategies all had shortcommings, but the justification was better feet than doing nothing.
 There were stunning successes with casts + manipulation
methods but it was a percentage thing. Some were great. Some were, after concerted effort, left as if untreated. Between these extremes was the range of most outcomes.
There were stunning successes with casts + manipulation
methods but it was a percentage thing. Some were great. Some were, after concerted effort, left as if untreated. Between these extremes was the range of most outcomes.
It was clear enough, very aggressive and early (immediate) manipulation of club feet on day one of life and thereafter did best. But, still, many very stiff feet did not yield. One noted practitioner urged
frequent manipulations and very skilled cast applications - each time performed under anesthesia. Multiple aggressive manipulations and anesthesia sessions, led to many better feet, yet many failures persisted.
In recent years, this concept has been revisited with continuous passive motion machines and splinting with some success. Limited lengthening of a posterior tendon may be used to boost the process. The formula is still essentially the more movement and holding in the direction of correction the better - for some feet, more feet, but still, not all of them. Botulinum toxin has been used for paralytic versions of clubbed feet with some success. Recently a similar usage was reported from Texas Scottish Rite Childrens Hospital. It is yet another way to create suppleness in the shortened tissues.
Even in the most aggressively conservative hands, the surgical rate was about 40%. Critics also argued that even in the 60% of successes, were many "questionable" feet. It depends on the criteria. If patient satisfaction was "glad not to need amputations" then the 60% rating was solid. But if the criteria included willingness to show bare feet on a public beech, or engage in sports, then another lesser statistic emerges. It comes down to "pursuit of happiness". What does that take? Avoiding surgery? Surgery? Or just plain outcome? Throw in risk. It is fear of the latter that has parents looking for conservative choices, even if monumental in scope and unequal to surgery in outcomes. Pursuit of happiness... but whose?
For feet that resist manipulative correction the surgical question was "Just what needs to be released to get a real, not just a partial or semicosmetic correction?"
 The answer turned out to be
"Everything". Club foot surgery essentially divides all the ligaments connecting the foot bones and lengthens all the tendons to allow total mobility.
The answer turned out to be
"Everything". Club foot surgery essentially divides all the ligaments connecting the foot bones and lengthens all the tendons to allow total mobility.
With that strategy, as was championed by Dr. Turco, real corrections are now possible. With that insight an array of me-too variations touting one skin incision over another flooded the reporting. Despite the rhetoric, the modern operations stress completeness. Some surgeons remind us of rotational needs, other stress bone column geometry, but to get there you have to disconnect a lot of stiff stuff.
"Corrections", of bone position and foot shape. But growth? It is still a club foot, no?
Of the feet that come to surgery (60% of them) 40% of those come to surgery again. A "corrected" club foot that is just let loose to go its own way will do exactly that. Its
own way is clubbed. Some sort of maintenance foot wear is recommended in the very early years after correction. The kids are too young to mind and the potential for recurrence too great to ignore. Nowadays we expect all club feet to look good and be functional. The one unsolved issue is the
smaller size of both foot and calf. When both feet are club feet, size is not a problem. But one sided club foot may result in ½ to 2 sizes difference. There are shoe and insert tricks to deal with this.
But size equalization is not yet solved.
Nowadays we expect all club feet to look good and be functional. The one unsolved issue is the
smaller size of both foot and calf. When both feet are club feet, size is not a problem. But one sided club foot may result in ½ to 2 sizes difference. There are shoe and insert tricks to deal with this.
But size equalization is not yet solved.
 However, it is a big world. Strange things can
walk in... such as these feet:
However, it is a big world. Strange things can
walk in... such as these feet:
This 12 year old boy was walking on these club feet. Note the knobs on what is anatomically the foot top but which is his weight bearing area. He trips and hurts himself, he said.
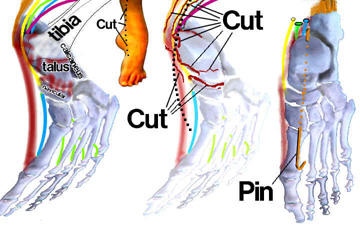
Attempts to straighten these feet included pins through the feet and through the shins to large metal rings with turn buckle parts which were dialed out progressively, until...
until his shin bone broke, actually both tibias broke! Of course they had to be allowed to heal. He has scars (you can see one on the right ankle area) from earlier failed releases done several times. Releases & Ilazarov frames did not even slightly correct these feet. There is nothing that ALWAYS works. In this case neither side budged.
 Back to prosthetics?
Back to prosthetics?
No.
Surgery for correction isn't all that's new. There is also "salvage" surgery.
Rather than remove the foot, we can remove internal substance to generate space and mobility to help the nastiest looking feet. These are the same feet as above. The youngster is getting about fine. The lump of thickened
skin, that served as his heel, is shrinking by the week. We can still see some of that thickened skin on the outer side of the ankle above. This was done in a short single step operation. No
external metal. By hollowing out the talus the heel can be counter shaped and placed inside - easily (talo-calcaneal intussuseption). X-rays look weird but the feet look fine and work.
 |
So, what did we learn? Beware of slogans. There is easy stuff and there is difficult stuff. No one method, so & so's exercise, the wachamacallit brace, the whoozie's operation, whatever - no one method is appropriate for the full range of problems that we see.
 |
Macrodactyly is a focal gigantism present at birth but progressive. Sometimes a single digit will grow to enormous size. One of our children had a toe as long and as wide as the rest of the foot. It is variable in the extent and degree of soft tissue enlargement. The latter can wedge the foot apart and thus deform the uninvolved bones.
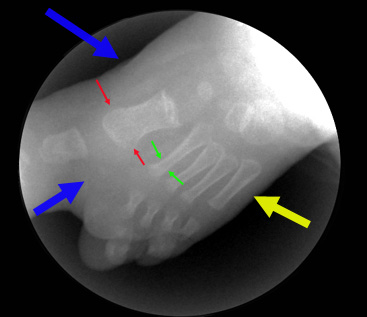 The x-ray to the right shows a
toddler's foot. The great toe is longer than the foot. The toe bones and the metatarsal (between red arrows) are very wide. Normal width is seen between the green arrows. The yellow arrow points out normal
skin thickness. The blue arrows point out the excessive tissue that triples the thickness of the foot and which wedges the second toe off in the wrong direction.
The x-ray to the right shows a
toddler's foot. The great toe is longer than the foot. The toe bones and the metatarsal (between red arrows) are very wide. Normal width is seen between the green arrows. The yellow arrow points out normal
skin thickness. The blue arrows point out the excessive tissue that triples the thickness of the foot and which wedges the second toe off in the wrong direction.
 As with severe club foot, many places used to and still do amputate the abnormal parts of the foot. In that case the great toe and its metatarsal would go. We prefer staged
growth arrests (to stop linear growth with segment removal to aim at mature length (to grow into) with mass reduction. That includes narrowing oversized bones by
longitudinal section. The lengthy process of staging an ultimate foot match makes some folks prefer amputation. It depends quite a bit on how much of the mid foot is involved.
As with severe club foot, many places used to and still do amputate the abnormal parts of the foot. In that case the great toe and its metatarsal would go. We prefer staged
growth arrests (to stop linear growth with segment removal to aim at mature length (to grow into) with mass reduction. That includes narrowing oversized bones by
longitudinal section. The lengthy process of staging an ultimate foot match makes some folks prefer amputation. It depends quite a bit on how much of the mid foot is involved.
This same condition may involve fingers and hands.
 Ectromelia is a failure to form the central portion of the terminal limbs (hands &/or feet).
It may be a first case by spontaneous gene mutation, however, most have an involved parent as it is a genetic disorder.
Ectromelia is a failure to form the central portion of the terminal limbs (hands &/or feet).
It may be a first case by spontaneous gene mutation, however, most have an involved parent as it is a genetic disorder.
Many have no difficulty with walking at all but
significant problems with shoe wear. Treatment problems are those of timing. These feet can be closed up to look fairly reasonable. However,
avoiding growth arrest in the process is important. Many wait until maturity for definitive reconstruction. Interestingly, many of those who do wait find that they really are OK with it and elect to let the feet be.
Our advise is to base decision making on function. If function is a problem, examine to see what specifically is interfering with the needed processes of walking. Address those items. That may well be something other than a cosmetic attack. For example, an orthotic-prosthetic hybrid may be fabricated which extends the foot rolling point forward to where a foot should have a rolling line (metatarsal heads). Depending on how much tissue exists, the reconstructive approach might not match the prosthetic extension in ability to further walking mechanics. Each case needs individual consideration of all the issues.
There are other methods for the intermediate problems. There are other ways to deal with the relapsed club feet that are not discussed here. The particulars get too particular for those. Just know that there are many tools in the tool chest.