 |
|
|
|
|
||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||
|
The Humerus The humerus is the arm bone (most folks call it the UPPER arm bone). It has action at the shoulder joint and at the elbow joints (two at the elbow). |
|
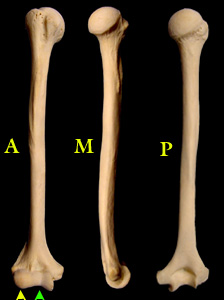
Seen at the right from the front (A=anterior), inner (M=medial) surface Notice that at the lower end seen from the front we see two joints straight on (two arrow heads). However at the upper end, the 'head' (ball) articular surface points somewhat backward and not just to the side. This is fitting as the scapula continues on in that oblique direction. The term for this is retroversion. In the leg the point from which we measure twists is the knee. In the arm we measure from the elbow. Using the axis of the elbow - as though it were a hinge - we define the zero axis. The humeral head points behind that axis just as the femoral head in the leg point forward of that defined axis (anteversion). Think quadruped. All the upper axes point toward the belly button (kinda sorta).
Vertically in front is an obvious furrow sitting between two bumps. The furrow houses the biceps tendon which passes over the humeral head to attach to the top of the glenoid. See? Tension in the biceps tenses a band (the tendon) above the head of the shoulder joint that assists keeping the head from slipping upward when lifting tension is strong. The opposite muscle from the biceps is the triceps. It attaches to the bottom of the glenoid. A pattern emerges. Combined tension of pairs of muscle stabilize the joint. The two bumps are handles for shoulder muscles, enhancing their leverage. The deep plane muscles of the shoulder attach with tendons that essentially join side by side into one continuous cuff - the rotator cuff. The forward surface of the scapula (near the ribs) is covered by the subscapularis which has forward attachment on the humerus just to the inner side of the lesser bump (the lesser tuberosity). The back surface has muscles from above the horizontal ridge or spine (supraspinatus) and below the ridge (infraspinatus) converging on the cuff tendon which attaches to the top of the humerus at the greater tuberosity and thence backward and down. That's another set : supra + infra spinatus (out & up rotation) vs. subscapularis (down & inward rotation). They are not alone. From the outer edge of the scapula more muscle joins the rotator cuff but acts much like the spinatus muscle
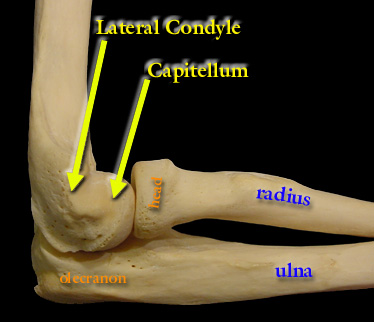
But remember, in children the bone might not be wholly made of bone. Parts may still be made of cartilage. At the lower end, for example, the bone that exists in reality a a single firm structure, may appear shorter with a round small bone beyond it when seen on x-ray. The capitellum, the round joint surface for the radius is not seen on x-ray until about two years old. Then a blood vessel penetrates the cartilage and begins branching and converting the center of that region to bone. That nucleus of bone (ossific nucleus) enlarges by converting the surrounding cartilage in which it is carried. The cartilage surface is retained as cartilage for articulation. We can tell the approximate age of a child from the degree of bone replacement of cartilage on x-ray. Approximately : the capitellum 'appears' at 2, the radial head at 4, the medial condyle at 6, the trochlea at 8, the olecranon at 10 and the lateral condyle at 12 years of age ("crimtol" or CRMTOL, 2,4,6,8,10,12).
The wrist and finger extensor muscles (straighten the wrist and fingers) attach as a group to the lateral condyle. The wrist and finger flexors (curl the wrist and fingers) attach as a group to the medial condyle. The radius turns on an axis that, at the elbow, passes through the center of the capitellum and, at the wrist, passes between the radius and ulna. Thus at the wrist the radius orbits the ulna as the moon orbits the earth (with same side facing). At the elbow the radius is in a constant relative to the ulna but showing a different surface as it turns. See forearm for more on this.
The elbow flexion and extension of the elbow, the thing we associate with elbowness, comes from the ulna to humerus articulation. Se elbow for details. But notice that the big groove (fossa in Latin) in the back of the lower humerus - the olecranon fossa - has to accept the olecranon when the elbow extends. When fractures deposit healing bone in this fossa, the elbow is limited in extension. Forcing extension only irritates that bone and causes more to form. That is why we advise against elbow stretching exercises following trauma to this area.
Notice that on this right arm, from the back, the medial condyle is far more prominent Chronic pressure on this spot - say, a wheel chair sitter with elbow always resting on arm rest - can cause hand weakness and odd sensations.
|
|
|
||||||||||||||||||||
 , and the backside
, and the backside  The round head portion sits in the
glenoid - more on than in as the glenoid of the scapula is rather shallow.
The round head portion sits in the
glenoid - more on than in as the glenoid of the scapula is rather shallow.
 The condyles are kind of like
tuberosities in that they are bumps that stick out and are there for muscle attachment.
The condyles are kind of like
tuberosities in that they are bumps that stick out and are there for muscle attachment.  The main action for which we think of the elbow is
not pronation (palm down) nor supination (palm up) but it is involved in that process.
The main action for which we think of the elbow is
not pronation (palm down) nor supination (palm up) but it is involved in that process.