 |
|
|
|
|
||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||
|
The Thorax, The ribs, the breast bone(s), maybe the clavicles can be included here, too. |
|
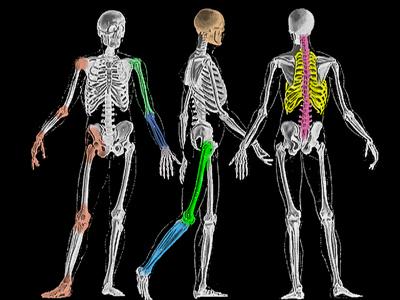
The thorax is a bellows bounded by ribs, spine, breast bones, and diaphragm.
Either way, they articulate with the manubrium at its very top edge. The first ribs sneak in under the collar bones (clavicles) to bracket the manubrium. The manubrium is the top of three breast bones. It ends just above the second ribs. Most of the breast bone is the sternum. The last rib to directly articulate with the sternum is the seventh. Below the sternum is a hangy down bone nubbin called the xiphoid. Its main function is to terrify parents into thinking it is a tumor. "What's this bump?" This is especially true when the youngster is thin and when the sternum is spoon shaped pointing the xiphoid forwardish rather than down. Ribs 8, 9, and 10 do a congo line thing to the prior rib. Ribs 11 and 12 float. The ribs become cartilage as they approach the breast bones. The green stars (*) show the approximate transition points from bone to cartilage. That cartilage allows more flexibility. The Bellows: When the chest expands, the lungs expand as well by the vacuum created. If the chest were perforated, the lung would collapse even though the chest wall were expanded as the vacuum between chest wall and lung would fail. If the lung itself perforates, the vacuum would fail. That too, would cause lung collapse. There are conditions which predispose to spontaneous holes in the lung that cause collapse. A plug any branch of the tree of pipes that deliver air to the lungs will collapse the lung that is supplied by that plumbing. In this instance, not from leakage but from absorption as the air gets transported from the blocked portion and, therefore, it deflates. Normally a full sized person moves about half a quart of air per breath cycle (in-out). That is the tidal volume - like the tides - the amount normally expected to flow in and out. The lungs are capable of about three additional quarts of air beyond the usual restful inspiration. This is inspiratory reserve volume. We breathe out. The expiratory residual volume is the amount of air left in the lungs after a fullest out breathing. A full sized person has a bit more than a quart of air in the lungs with a fullest exhalation. Vital capacity is tidal volume plus functional residual capacity. This is an orthopedic site, why is this here? Scoliosis. When spinal deformity twists the thoracic structures, the bellows may be stepwise diminished. That diminishment is carved out of the inspiratory reserve. The tidal volume keeps borrowing from the reserve --- until there is no more reserve. It varies with body shape and underlying conditions, but at about 40o of thoracic scoliosis, the reserve begins to be called upon for regular breathing. By 80o it is spent. After 80 degrees, each further increase in curvature reflects in a drop on pO2 measurement (a measure of oxygen carried in the blood). Another key issue of lungs in the neurologic disorders is reflux and aspiration. That food and gastric acid don't belong in the lungs is pretty obvious. How to detect and prevent that is definitely an issue, but not for here. Sorry. There is only so much space allotted us.
|
|
|
||||||||||||||||||||
 Depending on how
picky you want to be, you can include or exclude the clavicles. If you are a comparative anatomist, the clavicles if joined in midline (with the next item) are the wish bone.
Depending on how
picky you want to be, you can include or exclude the clavicles. If you are a comparative anatomist, the clavicles if joined in midline (with the next item) are the wish bone.