 |
|
|
|
|
||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||
|
The shin is the region of the tibia. At the proximal (in proximity to the body) is the knee. At the distal end (distant from the body) is the ankle. Nobody uses the distinction of 'leg' or foreleg to mean only a portion of the full leg from hip to toes. Well, veterinarians might. |
|
The lower leg is the place where the shin is found. Let's review some basic terminology as there isn't a whole bunch to say.
physis = the plate of cartilage near the end that metaphysis = the funnel shaped spongy bone
diaphysis = the shaft (dia = away from)
Pronunciation: physis = FY sis physes (plural) = FY seez metaphysis = meh TAFF uh SIS diaphysis = dy AFF uh SIS
<= This is the lower end metaphysis. The lower tibia and fibula epiphyses form the lumps that we see and feel at the sides of our ankles and call ankle bones. The fancy name is malleolus (mah LEE o LUS). The medial malleolus is the inner ankle bone and the lateral malleolus is the outer ankle bone. Together they are the malleoli (mah LEE o LYE).
The squarish and cylindrical shaped space between the malleoli is the mortise.
That axis is not parallel to the knee joint axis, but slants backward Now it gets a wee confusing. The axis of the knee is defined as neutral. We measure hip and ankle relative to the knee zero axis. Fine. However, tibial torsion - a condition in which the axis of the ankle defined by the mortise is a term that implies a twist of the tibia bone and thus ignores the femur. Sometimes that works and sometimes not. Frankly we have no idea what folks are talking about unless we back up and say, "Yo, what are you talking about?" [You can leave out the "Yo" part if you don't live in New Jersey.] Is this important? Ehhhh ... to parents it seems to be. But to surgeons the distinction is vital. The inward deviation of the ankle ( medial malleolus going behind the lateral) seen in toddlers (toe in) normally and gradually reduces spontaneously by way of growth mechanisms which read the forces delivered by running, walking, skipping, kicking stuff and activity in general. Resolution of tibial torsion will be complete by 5 years of age. But there are exceptions. Maybe the tissues just don't get it. That is the case in club feet not uncommonly. The torsion of the tibia may well simply fail to undo with growth. Many surgeons advocate a helpful bracing nudge during the early years to get that part of the syndrome (which is NOT confined to the foot) under control. In spasticity the bone may get mixed messages due to strangeness of function. It may go the wrong way and twist more rather than less - or - as the walking pattern imposes harsh forces, go the right way but too far. But some children twist late through the knee joint. That is, the apparent torsion is NOT of the tibia shape, that is, within the bone but of the tibia orientation (direction as a whole) relative to the femur through the knee joint. The medial hamstring pull, if harsh and unrelenting, can sublux the medial tibial plateau backward which points it and everything below it inward. Treating the muscle imbalance issue directly treats this malrotation. You have to pay attention to the details. Another detail is that a whole bunch of rotation can take place below the ankle through the joint that sits beneath the 'ankle bone' - the sub ankle joint (next section).
|
|
|
||||||||||||||||||||
 epiphysis = growing joint end that sits on the
epiphysis = growing joint end that sits on the
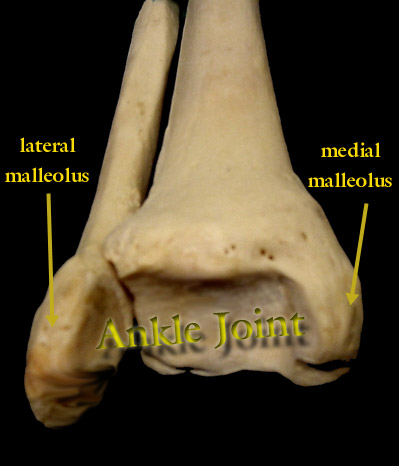 The tip of each malleolus has a short ligament which attaches to the ankle bone like a corn-on-the-cob handle. So the axis of the ankle is tip to tip medial malleolus to lateral malleolus.
The tip of each malleolus has a short ligament which attaches to the ankle bone like a corn-on-the-cob handle. So the axis of the ankle is tip to tip medial malleolus to lateral malleolus.