|
|
|
|
|
||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||
|
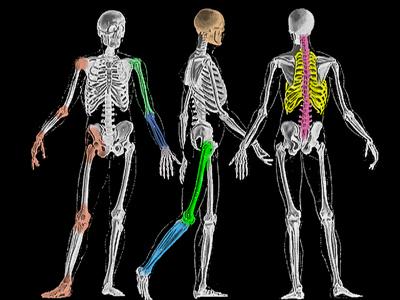
The knee is a region and the knee is a joint. As a joint it is made up of uh... how many bones ? Mmm... well, mmm, that depends if you want to count the fibula in on the action. Yeah, let's do that because it anchors the lateral ligament complex. The femur, and tibia are obvious . Add the patella and the fibula, that's four.
|
|
The patella is another name for knee cap. The patella tendon joins the lower edge of the patella with the tibia at a bump handle called the tibial tubercle (t.t.). Upward pull of a shared or joined tendon (quadriceps tendon) attached along the top of the patella comes from the 4 anterior thigh muscles collectively called the quadriceps. The wedge shaped patella rides in the femoral groove and thus serves to keep the extensor muscle from flipping off to either side as the knee bends. Therefore, the quadriceps pulls on the tibial tubercle via a flexible centering linkage (patella and patellar tendon). If the patella tendon were bone and the fibula made its way to reach the lateral condyle of the femur, then you have - more or less - an elbow. So, why a patella tendon? Well, the range of motion at the elbow requires big notches carved into the humerus to accommodate the olecranon (the elbow's patella + patella + tendon) . That won't work under the loads that leg bear. Thus arm triceps has homology to leg quadriceps, humerus to femur, tulna to tibia, radius to fibula.
Looking at knee motion from the side, though, gets tricky. There is an approximate "center" of motion through the femur ( * ). It is a moving center, though, for several reasons. Firstly the distal femur is not round - roundish, but cam shaped. The cam portions are called the condyles. There are two condyles, the medial condyle and the lateral condyle. Secondly, the two cams do not roll but rather roll and slide on the tibia below. The medial and lateral condyles do not slide equally - but that's a bit much for us here. The knee flexion axis traces through a short smile never far from what is shown here =>. Overall the stabilizing structures, other than muscle power, are cups and X's. The X's run from forward or back on the tibia to attach to the femur near that axis. Bands, as ligaments, more like straps than ropes, do the cris crossing. Further these straps twist from origin to insertion. That is a common theme with ligaments and many tendons. Fibers which start off in the leading edge at one point may become a hind edge of that tendon or ligament at another point.
This is a good design trick that allows differential tension through motion. Between the condyles the cruciate ligaments follow this plan within their structure. Grossly, they run from posterior and anterior on the tibia to the notch between the condyles. But it incorrect to think that only the cruciate ligaments are cruciate (cross). They are the most cruciate. The ligaments on the sides of the femur - the collateral ligaments (so named because bookies take them for collateral?) - also lean along this plan. The medial and lateral collateral ligaments do not run plumb up and down between tibia and femur, but along a sloped scheme. Having wider bases of attachment below (on the tibia medially and tibia-fibula laterally) allows those twisting bands to contribute to this strategy even more.
X's and Cups.
1) hyaline cartilage The smooth shiny and slippery surface of joints - the articular cartilage - that's hyaline cartilage (because of the way it looks under a microscope). The springy stuff that keeps your wind pipe open and makes the lung pipes so flexible - that's elastic cartilage. Your Adam's apple has that. The tough cartilage that is fiber reinforced to take a direct beating - that's fibro cartilage. The tangerine segment C shaped thingies that sit on top of the tibia to create a pair of cups in which the femoral condyles ride are made of fibrocartilage (the substance). Because "tangerine segment C shaped thingies" doesn't flow in sentences, folks just call them the "cartilages". These C-shaped shock absorbers expose a center of tibia joint surface hyaline cartilage. The medial one isn't exactly like the lateral one. Those details are not important here. What might be of interest is that instead of being C shaped, occasionally a meniscus winds up shaped like a checker - covering the whole side. That is a discoid meniscus. Kids may start out with a meniscus discoid and as it matures ( as the joint grows) it winds up right, C-shaped. These discoid cartilages tend to pop or clunk and wind up causing mommy to melt down thinking something awful is going on in there. A rare one - a very very rare one - persists in locking up the knee and requires being tailored.
The Tibia:
A = anterior P = posterior L = lateral M = medial The top of the tibia slopes downward from front to back. The front is like a face with a sloping forehead and a short button nose. That prominence is the tibial tubercle. The patella attaches to that by way of a tendon called the tibial tendon. When you look at that point where the quadriceps exerts its force and consider that approximate joint center on the femur then consider the distance to the foot --- gad! The leverage!!! That can easily be 10:1 and when you figure that the forces vary with the square of the acceleration - oh mihgod! A medium sized person can generate compressive forces of over a ton. Try this at home. Take a block of anything. Place a one ton weight on it. Now slide it. Oh, use ear plugs, forgot to mention that. How can this patella sliding in a groove work? Low friction. Very very very low friction. The friction of the patella on the femur is less than air hockey. The material of articular cartilage contains big spaces which house molecules that look like fish skeletons (or maybe like baby bottle brushes). Those hairy molecule ends all contain a sulfur based negative charge. Compression oozes those negative molecules out from both surfaces. Negative to negative! We ride on repulsive charge fields. Cool. But the molecules have to be put back. That takes energy and time. TIME. That's why repetitive knee exercises destroy knees. No time to recharge drags a ton block on a soft surface. Get it? It isn't basket ball that wrecks the knee. It's repetitive practice of jump jump jump jump jump etc. machine like without breaking up the pattern.
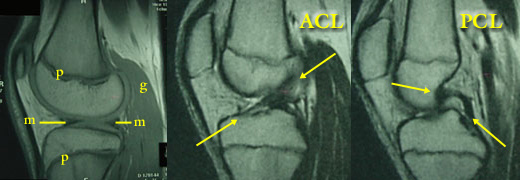
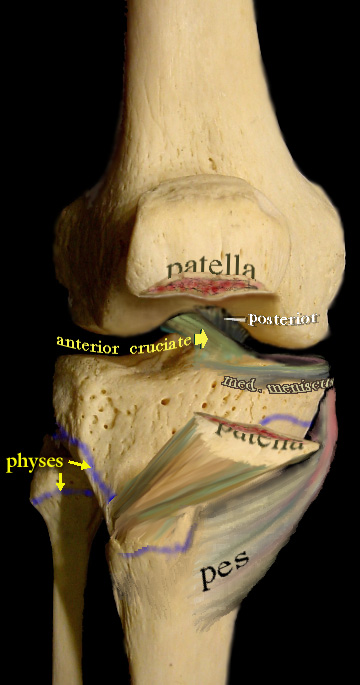
We see a blur demarcation line which shows where the physis of the tibia was situated (plural = physes, also showing that of the fibula). The growth plate of the distal femur is a horizontal line near the level where the top of the patella is in this image. The femur growth plate is nearly flat with a slight rise in the center and a gentle dip seen from the side. In contrast, the tibial growth plate sits like a Greek warrior's helmet (the kind with the nose guard) We see that the patella tendon attaches to a growth plate. Any epiphysis (bone sitting on the physis) that gives origin to a tendon (an epiphysis that gets pulled on) is called an apophysis. Apophyses all have one thing in common. They say ouchie a lot. There are the knee bump Osgood-Schlatter syndrome ouchies but there are also those of the heel, the iliac crest, the vertebral end plates etc etc. Each has a different name to make everybody confused. But the ouchies are like stress fractures. The pes anserine, which means duck's foot (No, really. No, really, it does mean that. Somebody thought the shape looked like a duck's foot) is an attachment of medial hamstrings to the tibia. More exactly three muscles share this one duck's foot (semitendinosus, gracilis, and the sartorius). The path of the semitendinosus is accentuated in this image to show that it flexes the knee but also can spin the tibia on the cruciates to produce a false inward twist of the tibia (intoe) in spastic conditions. The torsion caused by this mechanism is more prominent when the knee is extended than when fully flexed prone (which relieves the torque cause by the contracture). The anterior cruciate is seen running backward and outward to attach on the lateral condyle in the notch. We see, peeking above it, the posterior cruciate coming from the back edge of the joint to attach on the medial condyle - also in the notch.
MRI (magnetic resonance imaging) shows 3 side views at different depths (slices) Left Image : p= physis, m= meniscus, g= gastrocnemius, the condyle shape is well
seen and the surface articular cartilage on both tibia and femur are seen. Notice the small exposure of the tibia between the menisci > <. Also notice how the physis dips down
in the front of the tibia.
The cruciate ligaments can rupture, everybody has heard of that. But in children they are very strong. Much stronger than the bone. More commonly the injury that would tear a cruciate rips it off the tibia with a chunk of tibia attached - a "tibial spine fracture". Those can be wholly off, pulled up like a trap door on a hinge (no! chad goes the other way), or just a crack.
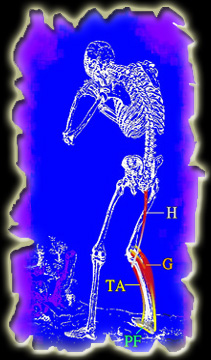
This is as good a place to discuss linkages as any. The knee is so central in linkage mechanisms. They are of two sorts : 1) mechanical The hamstring muscles (H) extend the hip and inwardly rotate the leg as part of the hamstring attachment is in front right next to the tibial tubercle. That also flexes the knee. So, the hamstring will flex the knee if the hip is stabilized or extend the hip if the knee is stabilized . But it can straighten the knee if the hip is allowed to extend but the foot is linked to the floor. The gastrocnemius muscles (G) are thought of as plantarflexors (point the foot down). But if the foot is stabilized, the attachment of the gastrocnemius muscles above the condyles of the femur allow the gastrocnemius muscles to flex the knee. If the foot is not stabilized by the ground in this respect, it can be stabilized by the tibialis anterior (TA) - a foot puller upper. But the TA is small and the gastrocs big. For that to work, the leverage must be set just so. One way is to highly and early dorsiflex the foot so that the heel attachment is nearly in a straight line with the tibia. The plantar fascia (PF) which spans the arch of the foot becomes a passive tension strut in this linkage. This is how using a hamstring exercise machine can give plantar fasciitis when the weights are too heavy. Strong assist from gastrocs kicks in and recruits this linkage. Thus the tibialis can be listed as a knee flexor. Hmmmmm. There are many such muscle linkages in normal function. The same linkages are also sensory linkages. Tension developed in the tibialis anterior may be developed from afar. This is important in considering control in conditions with sensory loss. Fusions might blind these islands of sensory integrity. Less stable stabilization may result in better control via better sensibility.
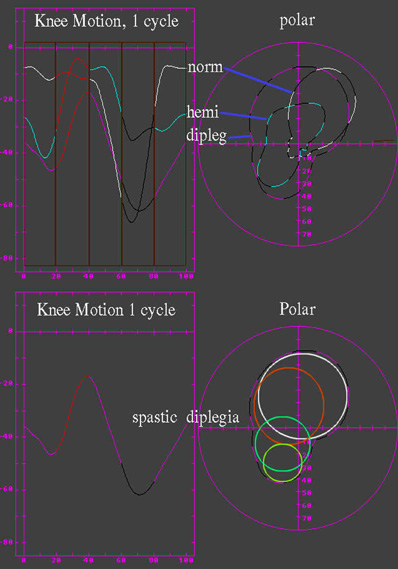
Knee motion plotted as a polar graph is far more sensitive in picking out the contributory components of knee motion. In the graph of "normal" the main trace is an ellipse. An ellipse is a circle with two mathematical centers (hip and knee mechanisms cooperate in knee movement). A third smaller action is seen - that from the foot. In abnormal gait, what we see is not abnormality carved into or out of the normal pattern - but rather different usage of the intact parts. Their signatures (size and angular speed alias amplitude and period) give them away. The pattern seen in spastic diplegia wherein a crouch rotated gait still allows a frisky scamper across the room - reveals a clever usage of the usual parts but in smaller sequential combinations. What looks wrong isn't what is wrong but what is making due in the face of what's wrong.
The key to normal movement is supple motion with easy short muscular contribution. When that fails, momentum ceases to be an effective mechanism and mechanisms must stabilize. Stabilizing mechanisms call on stabilizing linkages. A fully extended hip stabilizes on the hip capsule. The knee stabilizes on its ligaments in a bit of hyperextension. When sensation causes instability by defeating timing, the process gets noisy and rough as the mechanisms generate feedback through noise (slam slam slam) and jarring. Sensory loss produces profound destruction of joints, especially ankle and knee.
|
|
|
||||||||||||||||||||
 The knee is not a hinge even though it looks as though it moves that
way.
The knee is not a hinge even though it looks as though it moves that
way.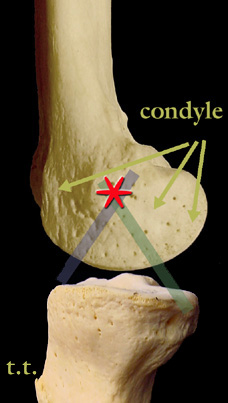 Easy enough, huh?
Easy enough, huh?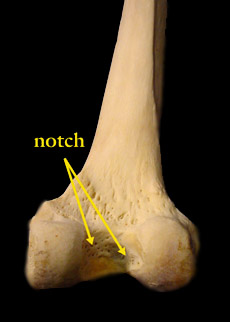 .._______
.._______ The cups. Gee. The tibia top doesn't look cup shaped. The top two bearing surfaces (
The cups. Gee. The tibia top doesn't look cup shaped. The top two bearing surfaces (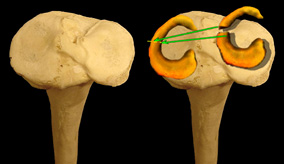 That's where the cartilages come in.
First the confusing terminology. There are three totally discrete things called cartilage:
That's where the cartilages come in.
First the confusing terminology. There are three totally discrete things called cartilage: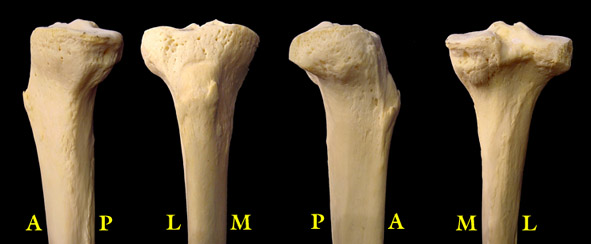
 Here we see the knee with the patella split
horizontally (as in a transverse or horizontal fracture). The lower piece of knee cap is swung downward attached to the patella tendon. That tendon attaches to the tibia at the tibial tubercle.
Here we see the knee with the patella split
horizontally (as in a transverse or horizontal fracture). The lower piece of knee cap is swung downward attached to the patella tendon. That tendon attaches to the tibia at the tibial tubercle.