|
Paralytic Hip Dysplasia
Augmentation Acetabuloplasty
Hip socket augmentation is performed for a variety of reasons. The most common, in handicapped persons, is to deal with a dislocating hip or subluxing hip.
Dislocation means that the hip ball at the top of the femur bone (thigh bone) slides
right out of the socket altogether. Subluxation means that the ball moves from its normal centered position toward the potential of dislocation, but not over the socket edge altogether.
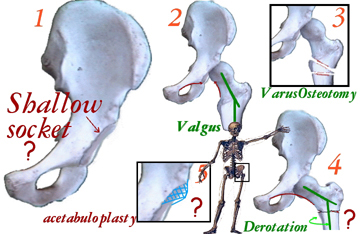
In that setting the hip dislocates because the hip socket is too shallow (1) and too vertical (1). The upper end of thigh bone might also be insufficiently angled (2 =
'valgus'). Cutting the thigh bone to angle the upper femur more sharply into the socket is be used at times. The disadvantage is that this femur surgery (3 = Varus osteotomy or VRO etc.) shortens the leg and causes the leg to track oddly between
sitting posture to standing. Healing to standing time is about 12 weeks. A hip metal 'nail' is needed and is removed about one year later. Loss of position is not
rare, requiring potential revision surgery.
'Innominate' (or pelvis) osteotomy repositions the hip socket itself by cutting the pelvis and swinging the socket to a new orientation - more horizontal. A wedge bone graft is used to set the new configuration. Threaded pins hold the graft. Leg length is
not changed much, as the shift occurs nearly through the center axis of the hip itself.
Some cases can be dealt with by merely building out the edge of the hip socket (acetabuloplasty = 5). Bone from the pelvis and/or from bank sources is used. This does not bring new joint surface to the built up area but merely enhances stability in
the existing articulation region. It is well suited to cases of early hip 'migration, in conditions of lesser demand - limited function, household ambulators etc. Alone, it
seldom requires blood transfusion. If a body cast is used (many do not need it), it is removed in about 4 to 6 weeks. See Cafe' Door surgery for a very special kind.
Lengthening the 'ileopsoas' muscle is occasionally needed (inside the pelvis). This intra-abdominal surgery can elicit a normal trauma-survival intestinal shutdown reflex
called "ileus". Ileus lasts from minutes to several days. It requires feeding by intravenous route until that protective reflex subsides. Additional muscle surgeries,
such as lengthenings are done to deal with the paralytic causes and to attack functional needs as indicated case by case.
|