|
Prevention
of Hip Problems
DDH
CDH
Paralytic
Hip Dysplasia
"An ounce of prevention is worth a pound of cure."
[B. Franklin] This is about as true a truism as can be found.
The hip is a ball & socket joint. Genetically joints are formed with the information of shape on one side (this case the ball), and the ability to conform in shape on the
other side (in hip's case, the socket). So there is a ball on the upper end of the femur and a zone on the side of the pelvis that can shape to the ball, creating a socket.
 The conformable socket tissue
is cartilage, not bone. In the image at left, the unseen (on x-ray) adaptive cartilage of the socket is depicted in orange. The unretouched x-ray is on
the left. Notice that one visually underestimates the hip socket and ball dimensions because the cartilage components are unseen. They can be viewed with ultrasound, however. The conformable socket tissue
is cartilage, not bone. In the image at left, the unseen (on x-ray) adaptive cartilage of the socket is depicted in orange. The unretouched x-ray is on
the left. Notice that one visually underestimates the hip socket and ball dimensions because the cartilage components are unseen. They can be viewed with ultrasound, however.
Note that the sharp upper edge of the socket is like an awning. It covers the ball and points downward and outward. Growth follows that edge, downward and outward.
Thus the hip gets deeper as it grows taller with the ball. But that tissue is soft, like your ear. If the hip ball slams repeatedly upward and outward (very apt to do so
with the legs crossed), then the soft cartilage, like a boxer's nose, gets flattened. It gets flattened upward.
With the leading edge growing upward, the socket becomes taller beyond that of its
own inner wall growth and becomes more vertical. It becomes vertical and shallow. The socket cup, by way of disoriented growth, becomes a dish, a shallow dish. The
slope of motion of the ball in that dish only slams the upper edge more. The ball, under muscle tension migrates steadily upward and out over the poorly containing
edge. Subluxation (migration from centered position) evolves into dislocation (hip out of the socket altogether.
The x-ray image on the right shows the largely unseen ball of the infant hip (which
is also cartilage - but tougher) in yellow. One hip is "located" (centered where it belongs) and the opposite hip is "dislocated".
DDH:
If pressure in the womb presses the fetal leg too severely, the socket can flatten. It may well go unnoticed. The softer the cartilage (girls are softer because they react
to mom's hormones) and the more the push (usually the left leg gets it worse as it is usually up against the spine), the more the odds of a flattened socket. Girl babies
get hip dysplasia (socket flattening) 9 times more than boys. Breech position is just plain nasty to the hips and squashes hips about a third of the time.
Unless aggravated, small amounts of flattening might resolve spontaneously.
Cultures that carry babies with the child's legs spread apart, such as riding on the mother's hip, have, by far, the lowest incidence of hips that go on to be bad. African mothers have the best track record of all. Their protective way of carrying babies is unbeaten - held in an open-legged position by a sling-bandana. Cultures
that wrap legs together in one way or another (swaddling etc.) just plain destroy hips. Swaddling of children leads to waddling adults.
The actual dislocation of the hip may well come about later. The initial loss of hip
edge integrity, with time, kicking, standing and life's forces leads to slow further degradation of hip relative depth with time. It may dislocate. It may just wear badly and become osteoarthritis is the young adult.
PARALYTIC HIP DYSPLASIA
Children with abnormal muscle forces around the hip do not need an abnormal
starting point to get their hips into trouble. Perpetual slamming forces that get directed outward on the socket edge come from overactive hip adductors and
hamstrings (hamstrings are not called "adductors" but are nevertheless powerful adducting muscles.
What is adduction? Cross your right leg over into left leg territory. That is adduction
. In that posture, pull along the axis of the thigh bone points right out of the socket.
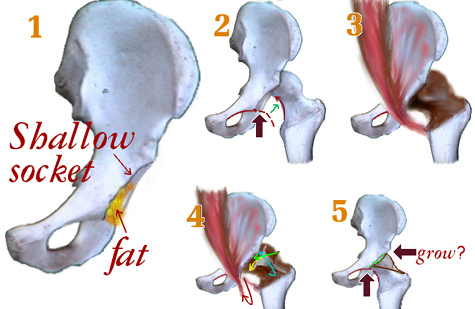
1) Pelvis (innominate bone) with the socket. At the bottom is some fat. If the hip displaces, the fat
enlarges and fills in. It is a tough gritty kind. It may block the hip from getting back.
2) A line along the lower edge of pubis lines up smoothly with the neck of the femur. If not, the femur
has drifted (subluxation or dislocation).
3) The hip capsule (brown) is a tough sleeve that covers the hip and keeps in the lubrication.
4) The iliopsoas muscle, if shortened from subluxation may well prevent getting the hip recentered. It often forces lengthening.
5) The cartilage top edge of the socket is paired with the top hip capsule quite closely. If it is
deformed from the awning down and out direction at the bone edge, it may need to be redirected if growth is to become reoriented.
A special adaptation of wheelchair positioning, "the Mary Chair" [also called Hip Safe Chair, or Happy Hips Chair] is also very helpful in the care of very spastic patients.
Prevention :
You have to be aware that nature can play dirty tricks. If there are risk factors such
as a family history of hip dysplasia; a baby that is born large, or mother is small (tight packaging, potential for odd-ball positions in the womb, especially breech); a
baby whose left leg seems to fall naturally along the body's midline rather than out to the sides - whatever - don't wait for waddling gait to react. Why? That ability of
the socket tissue to conform gets diminished with time. It is a bell-shaped curve thing. It may well be gone by age two! If the hip is very flattened and the child is
almost two, there may well be insufficient time to undo it. Some kids luck out and retain that growth reshaping capability to nearly 5 years, at least to some degree.
A simple harness that mimics the baby astride the mother (as mentioned above)
does well to let those hips reshape. But it is important to be certain.
 |
Children with paralytic diseases must simply be monitored. They can go from looking just fine to awful in very short periods of growth. It is especially
common to see hips go bad after an unrelated illness. Why? Anything that increases the muscular tone just increases the chances of the hips not being able to withstand
the pounding. We recommend, as a generality, that all children with cerebral palsy, for example, get a yearly x-ray of the pelvis for viewing hips.
Earlier detection of problems usually allows simpler and better remedies.
|