|
Slipped Capital Femoral Epiphysis
(SCFE)
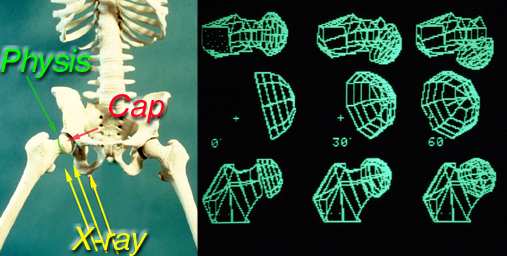
The femur has two major growth regions. 1) at the bottom near the knee and 2) at
the top, the cap, at the hip. The ball of the hip is actually a half sphere and caps the femur. The cap is connected to the rest of the femur by a disc-shaped cartilaginous
growth-zone region (growth zone or plate = "physis", on top of physis = epi-physis). This cartilaginous growth plate is not as hard or as stiff as bone but has the ability to add length to bones.
SCFE is one of the most common of the major disorders of the hip in adolescence.
It affects boys somewhat more than girls. The usual age is about ten to sixteen years old. It will usually involve one side, but may occasionally be bilateral (both sides).
It is a displacement (slip) of the capital femoral epiphysis from the rest of the femur through the pliable cartilage growth plate (physis).
The capital femoral epiphysis is the ball of the hip joint while the acetabulum is the
socket. In SCFE, the acetabulum, by embracing the femur head, helps shear off the femoral neck through the cartilage growth zone, especially if the cartilage is thick, if
the cartilage is soft, if the forces are high (big person, heavy or tall), and/or if an abnormal "fulcrum" is present (scarred soft tissue outside the bone).
The true cause of SCFE is unknown, although there are many theories. Most likely,
SCFE is caused by multiple factors including local trauma, obesity overcoming the physeal plate, inflammatory factors, and possible endocrine abnormalities. SCFE is
known to occur in association with hypothyroidism, panhypopituitaryism, gonadal conditions, renal osteodystrophy, and during growth hormone therapy. Endocrine
abnormalities should certainly be considered when a child presents with bilateral SCFE.
Having said that, most cases find no measurable link save for late maturation and
large size. Because the growth plate is cartilage, it is the softest part of a bone. In the young, it is a thick zone. In older kids, it is thin and irregular like the surface of the
moon. That irregularity may stabilize this very stressed piece of anatomy. If it remains thick, then those irregularities do little to lock the femoral cap undersurface
to the rest of the femur. Big (tall or fat) means more force to withstand.
A dense hip capsule (sheath) may also supply a fulcrum that the extending hip pulls
against to shear the cap off the femur (cap pushed back). There is a lot we still need to know as to why. But any illness that softens the cartilage or has it remain thick will predispose.
Commonly, children will complain of hip pain and a limp for some time, occasionally months. The pain is often not associated with any specific injury,
although it may increase in intensity from some minor trauma prompting the parents to take the child for an evaluation. Rarely, the pain is acute and intense beginning
after trauma to the hip. It is also common for children to complain of knee pain, which is referred from the hip. Any adolescent complaining of knee pain should also
undergo a thorough examination of his or her hips. Some will complain of groin pain. Some may even wind up with a urologist for a question of testicle pain.
As the physis, which is what actually fails structurally, is a soft material, it need not
actually split apart to fail. It can shear, ooze almost, move very slowly backward nudge after nudge and repair microscopically although displaced. This can be so
subtle as to cause no symptoms in a slow migration. Imagine two slices of bread connected by peanut butter. One slice can be displaced relative to the other without
any loss of continuity if it is slow enough. For the leg, the only sign may be that the knee (or foot) points more outward (slew footed) than before.
Thus, SCFE can be broken down into two categories: stable and unstable. A stable slip is defined as one where the child can still bear weight on the affected extremity.
They can do that if when it doesn't hurt severely. The implication is that the pieces have not actually pulled apart. There may be microfracture, but there is still intact connection.
A slip is considered unstable if the child cannot bear weight on that extremity. Pain indicates that the physis has split. That hurts. This has certain implications for the treatment and prognosis of the slip.
On physical examination, the child will have painful range of motion of the hip.
Rotation of the hip is especially limited. When the hip is flexed (with the knee bent), it will tend automatically rotate outward (knee cap points outward as the foot swings inward).
A physician can diagnose SCFE using an anterior–posterior (AP) and a frog lateral x
-ray of the pelvis. A landmark called "Klein's line" is used. Klein's line is an extension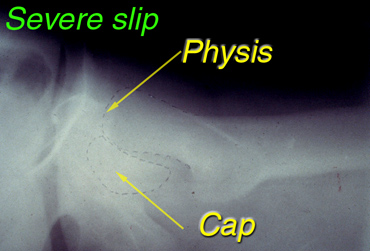 of a line drawn along the top border of the femoral neck. Normally, part of the femoral head will overlap this line. When a slip is present, the femoral head
will remain to the side this line, without any portion intersected. of a line drawn along the top border of the femoral neck. Normally, part of the femoral head will overlap this line. When a slip is present, the femoral head
will remain to the side this line, without any portion intersected.
When the diagnosis of SCFE is made, it is classified as either stable or unstable. We believe that a stable slip should be stabilized as soon as
possible so the child does not have the opportunity to transform a stable slip to an unstable slip. An unstable slip is even treated more urgently, as if it was a hip fracture. It is, actually, in a way.
 Nowadays, treatment of a SCFE usually consists of in
situ (just as it is) pinning using a cannulated screw introduced over a guide wire. The capital femoral epiphysis is not usually pushed to a more anatomical position for fear that it may compromise the blood
supply to he femoral head, causing avascular necrosis (death of the cap). An unstable SCFE is not forcibly reduced, but just positioning the leg for surgery may
diminish the slip a little. One or possibly two pins are used to stabilize the slipped cap. The cannulated screw will eventually cause the epiphyseal plate to fuse so that
the slip will not worsen. The use of multiple screws as seen below, is uncommon today. Nowadays, treatment of a SCFE usually consists of in
situ (just as it is) pinning using a cannulated screw introduced over a guide wire. The capital femoral epiphysis is not usually pushed to a more anatomical position for fear that it may compromise the blood
supply to he femoral head, causing avascular necrosis (death of the cap). An unstable SCFE is not forcibly reduced, but just positioning the leg for surgery may
diminish the slip a little. One or possibly two pins are used to stabilize the slipped cap. The cannulated screw will eventually cause the epiphyseal plate to fuse so that
the slip will not worsen. The use of multiple screws as seen below, is uncommon today.
Stable slips are usually treated without complication as long as the screw is inserte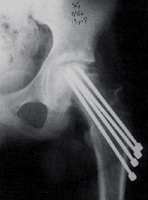 d in a central position. Since the slippage is not reduced, but
the cap pinned as is, the anatomy of the hip remains a bit different from the unaffected side. Although that hip will not be the same as the other side, the child should be able to
participate in all activities without pain after the growth plate heals by bone closure. X-rays are taken to assess that degree of healing. d in a central position. Since the slippage is not reduced, but
the cap pinned as is, the anatomy of the hip remains a bit different from the unaffected side. Although that hip will not be the same as the other side, the child should be able to
participate in all activities without pain after the growth plate heals by bone closure. X-rays are taken to assess that degree of healing.
Unstable slips have a much higher chance of developing complications. The most dreaded complication is avascular
necrosis. Avascular necrosis is loss of blood supply to the head of the femur (the cap), thereby causing the bone to die. It slowly weakens and collapses into
deformity. This may involve a portion of the femoral head or the entire femoral head. There are not many good options for treatment of this complication, so this
problem is best avoided. It can occur even if things go well, but is more likely if the slip is extreme or unstable. Avoidance of this outcome is the reason for not trying to
put the cap "back where it belongs", which carries a very large risk of avascularity.
|
