|
Cafe' Door ?? vs VRO??

Why another operation for the hip? There are so many already? That's a clue that what is out there isn't
wonderful. But beware. While we will assert that this SEEMS to be a better choice than some of the other "traditional" surgeries . . .
IT'S NEW! Wooowee!
But that means there is no long term assessment possible. We are riding on our gut instincts and the mechanics of it.
 The problem is that VRO thing. It was shown how conservative cast positioning for
congenital hip dislocation could be abbreviated by leaving the top of the femur abducted and inward rotated by cutting the bone to bring the rest of the legs together. The problem is that VRO thing. It was shown how conservative cast positioning for
congenital hip dislocation could be abbreviated by leaving the top of the femur abducted and inward rotated by cutting the bone to bring the rest of the legs together.
Given a late diagnosis of DDH and a potential several years in a nasty body cast holding a leg
in bizarre position, cutting the bone at the top let the part that needed to be that way - be that way - while the rest was more humanely positioned (held by metal
plate & screws etc). So the CAUSE was gone - uterus crush. The blue print for growth was perfect and young. Just get the pressure off the dent in the acetabulum and nature in good form will do the rest.
Ta-dahhhh. A hero operation! So when you have a great football team with huge linemen who won the trophy... do you just say attaboy to
them? No you send them off to swim the English channel. So big muscle guys with no body fat sink like stones and are never seen again?
What? The VRO - hero of newborn babies with a dislocated hip... was champ of baby hips and so sent into battle with spastic dystonia [which
takes perfectly normal hips and over time grinds them down and pulls them apart]. Go VRO! Go get'em!. Do do it like you do'd it in DDH!
But in DDH, VRO had no opposition. THAT was gone with birth. It was a sweep up job after the riot - not
during. In CP, hips are perfectly normal good hips that are being destroyed by force clashes that are still
ongoing and in excess of what the human natural blue print can endure! It's not the same. Fighting a war with a dust pan? And even if it did get things back, what stops more damage?
So VRO went off to fight another war, a different war. But did it do well anyway? Is it a hip lucky operation?
No. Failures abound. Rehab from the surgery itself is awful. We have data now from all kinds of really good
places (extensive data too) that tells us what any private surgeon would have known in a month... not good. How can you have so many failures (where there are few if any good outcomes and so much overt failure that
you have to reoperate are on the the majority) - how can there be that many failures and nobody notice it for over 50 years!!!!!!!! Come on! People in white coats. I blame you!! You refuse to acknowledge anything
unless there is 1000 of it.
Pig headed number worshipers. Have to have scores of ruined kids to satisfy 'p' value nonsense? And the
AACPDM presenters are adoring themselves over their scientificness and decimal places? They are still pushing this approach.
Yes. I am old and grouchy. Couldn't I say it nice? I guess but that was years ago. Ahem, hasn't anybody
noticed that this procedure is unstable in CP? Residents come & go and do NOT follow the outcomes - assuming everything they touch is golden. So the professors call for numbers. Oooo, not good. Maybe use
sharper tools. Do a thousand more. Nope. Do it younger. Worse. Another thousand. Do it older. But never: "Don't do it at all."
Then along comes a really cockamamie theory calling itself lever arms. Hey did you notice that the human body has bones?
Really?!
Yes and they act as levers.
Oooooo. Really? Do tell.
Yes and levers ,contain physics and you can name drop Newton. They come in three kinds: One two and
three. So cerebral palsy is when the levers get vectors that cause the levers to do naughty things.
You mean it isn't a neurologically driven muscle mediated process? So when baby seals are being battered it
is the club's fault? Damn them vectors! Cut all those leverage bones. Big cuts every where. Then call it "The
shark bite method". [Seriously that is the name]. Make sure you look doctorly. Gotta have a starched white
coat to get away with spewing that nonsense. Did anyone ever see an octopus escape by squeezing through a tiny hole? No bones. No bone vectors. Shape shifting out the wazoo. Explain.
Madam, your child is falling all over the place because she has vectors. We need to break all her bones.
NOT FUNNY!! NOT FUNNY AT ALL!! OK. I'll stop.
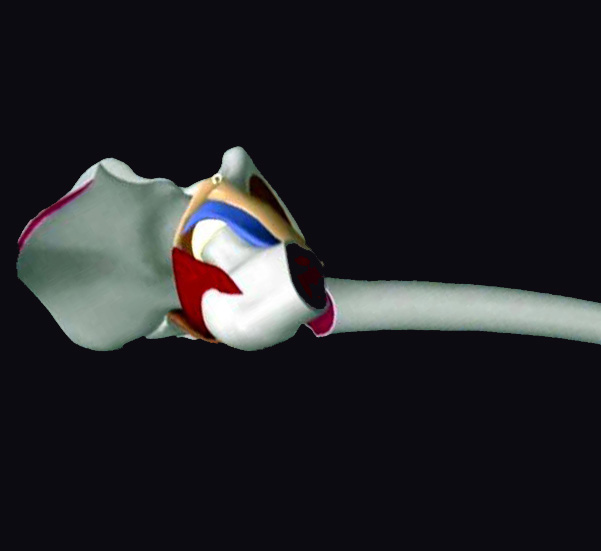
With VRO the surgeon does not even see the hip. [Top image right part]. She sees the greater trochanter
through a slit cut in the tensor and outer thigh muscle. The femur bone gets cut without seeing the socket at all,
without any clue of what is amiss in the shape of the socket or ball or ligaments. So, based on faith, tilt the top
end down with a bit of back rotation to take pressure off the front of the socket. Oooo wait? In DDH that is where the dent is.
In CP, is it? Yes? No?
No. The dent is usually on the back side. So is the R turning (the R in VRO for rotate) the turn the WRONG
way? mmmmmmmm... looks that way to me. But you wouldn't know, would you? You can't even see the hip ball or socket from here. There was a time when real hip surgeons actually looked at the hip itself. They
still do. [Top image left part]. They would look and see what is specifically wrong and hands on determine what specifically seems to make it behave better.
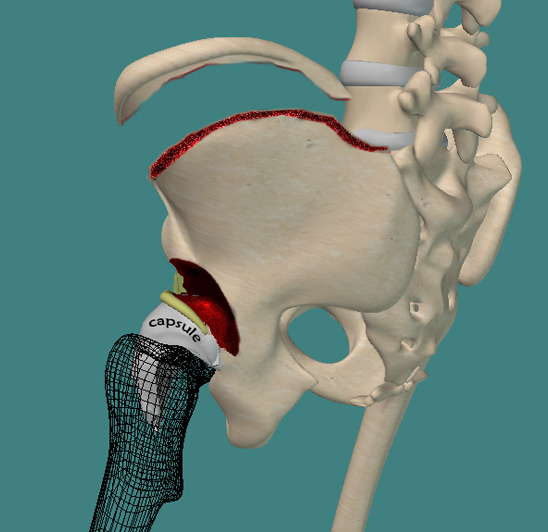 |
Click the above for a PDF of the surgical exposure for Cafe' Door.
Very graphic. Not for those weak of heart!
Whoa. That is not smaller surgery. No. Not at all. Best bet is don't let it get so bad that this is what we are led
to. Prevention. Do not wait for x-ray changes to rid a child of obviously potential damaging forces. You don't
kneel on a child's neck and require an x-ray of the wind pipe to determine whether to stop. Strong hip adduction forces with leg crossing and prolonged sitting damage hips. We have huge data that clearly shows
Botox doe not protect the hips. Indeed the love affair with Botox is making us awash in bad hips. We like Botox for lots of stuff but hip protection is nil.
The Scandinavian publishing gurus are pushing to just do nothing until certain changes are seen on x-ray. Joint
damage but the top professor actually denies that there is any damage to the hip if the x-ray shows displacement. Huh? Not proven with 'p' value that the hip is damaged. By the way there is no proof with
sufficient 'p' value that the bulk of buried Ebola victims are still dead. If you don't look for one will one just walk up to you and say "Hi. I am the 'p' value that says your shoelace is untied."
One of the most common and gravest errors in computer programming (and math) is to assume a specific
value in the absence of data. The rarest number of all in the natural world is zero. Assuming zero (something is not there) because of no study is not only wrong it is uneducated and stupid all rolled together.
However we need more experience and definitely much more time to know whether this method - which does
the initial intent well, (put the ball in the hole) does it well and without the immobility and long term convalescence. But will it prove to have been worth while.
|