|
Innominate Osteotomy
Chiari
Osteotomy
Salter Osteotomy
Pemberton Osteotomy
Sutherland Osteotomy
Steele Osteotomy
Dial Osteotomy
Dega Osteotomy
Peel Down
etc.
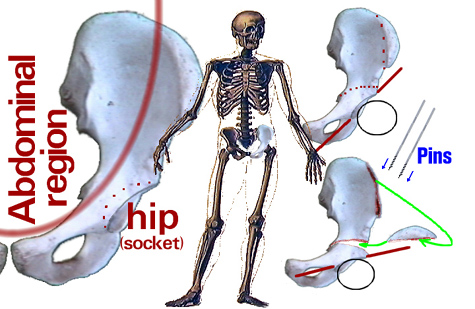
The hip may be too shallow to contain the ball of the hip. Not uncommonly that same hip is too vertical - the socket opening faces outward like the bowl of a
headlight rather than downward on the ball like a hat worn on the head - the norm is actually more like a beret, sitting at an angle.
Surgery that cuts clear through the pelvis is of several kinds. One kind strives to make a deeper socket. Chiari,
many years ago, developed a way to cut the pelvis just above the socket and push the socket inward so that the overhang of bone above would enhance the "coverage" of the ball. Steel pins to hold the slide position
are often used. Pelvis bone heals fast. Things are usually solid within four weeks.
The Chiari approach just covers the mature hip ball with raw bone, which lacks the slippery hip cartilage of a good socket. However, this was the first
really effective hip augmentation. Hip socket augmentation is done for a variety of reasons. The most common, in handicapped persons, is to deal with a dislocating hip. In that setting the hip dislocates
because the hip socket is too shallow and too vertical.
To try to get the shallow socket more over the top of the ball (more like a cap and less like an ear muff) another sort of pelvis cut is performed. Depending
on from where to where that cut is made, each version has a slightly different way it swings the socket. A very well liked straight cut version, the Salter Osteotomy, for certain kinds of pathology attempts to swing the socket more forward as well as a bit over the top. The bone pivots on the pubic symphysis..
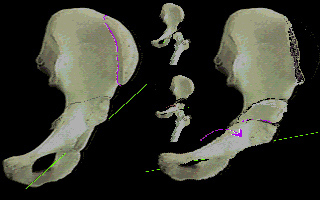 
Salter Osteotomy
Pemberton found that he could not get that cut to swing far enough to the side in the older
more neglected cases (Indian reservation) that he was dealing with. His cut takes a steep arcing curve, parallel to the socket, to allow a steeper over the top swing of the socket from
a lower pivot axis. That arc required that the growth zone in the hip be mature as it crossed where Salter avoided, a growing zone. Pappas devised a hybrid of the two for the in
between cases. Sutherland found that the pubic hinge, on which these operations rely, is
stiff in certain patients, so he added another bone division near the pubis so as to not depend on the suppleness of that structure. These surgeries are very similar, save for subtle
geometry shifts. They avoid crossing vascular supply. The Dega version is very similar but
pitched to favor more forward shift of the socket (for spasticity as compared to developmental hip dysplasia where the socket defect is forward).
Then the more aggressive surgeries were developed which, in various ways, essentially
carve the hip socket right out of the pelvis altogether and put it anywhere the surgeon pleases. The down side is that it may not be where the blood supply pleases, nor where stability of the result is as secure.
The general name for the three bones that make up the pelvic bone is innominate bones.
Altogether, these surgeries are grouped as innominate osteotomies (oste = bone, tome = cut).
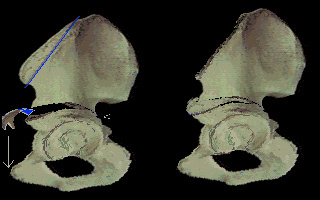
Recap:
Innominate' (or pelvis) osteotomy repositions the hip socket itself by cutting the pelvis and swinging the portion that has the socket to a new orientation - more horizontal. A
wedge bone graft is used to lock in the new configuration. Threaded pins hold the graft and socket until the bone bonds together. Leg length is not changed much, as the socket shift
occurs nearly through the center axis of the hip itself.
But note, socket depth is not changed at all. If the socket is far too shallow, a repositioning
strategy might merely convert upward dislocation to backward dislocation.
Shallowness can be dealt with by merely building out the edge of the hip socket or actually folding down the socket edge or both, acetabuloplasty. Bone from the pelvis and/or from
bank sources is used. This does not bring new joint surface to the built up area but merely enhances stability in the existing articulation region. It is well suited to cases of early hip
migration, in conditions of lesser demand - limited function, household ambulators etc.
When the cause of the poor growth of the hip socket to proper shape and depth is a
pounding by spastic muscle or otherwise high unremitting force, those issues are also dealt with. Lengthening the 'ileopsoas' muscle is occasionally needed. Additional muscle surgeries
, such as lengthenings or transfers may also be added to deal with paralytic causes and to attack functional needs as indicated case by case.
Many of the surgery types mentioned above require a body cast that includes the legs. If only pelvis bone is involved, four weeks is typical cast time.
Peel Down Procedures:
The innominate term refers to any of the three embryonic rib bones that join together to
form the bulk of the pelvis (minus sacrum). The three are ilium, pubis, & ishium. Each is an innominate bone. You sit on your ishium. You put your hands on your ilium. And you
get kicked in the pubis -oooooooooooh. Doh.
The bigger part is the ilium which makes up most of the wing or bowl of the pelvis. The hip
joint, however, is a circle centered where the three come together. All three have pretty substantial contribution to the socket (acetabulum). The roof of the socket os mostly the ilium. Review these bones?
OK, the above listed operations are some of those that cut through the pelvis bones to
reorient a portion - say - to make the socket more of a roof than a doorway. The peel down surgery instead cuts INTO the innominate (ilium typically but not exclusively) to
reshape the cup portion within that portion of the pelvis. This leaves gaps that need to be filled (bone grafted). The contour changes do make the actual socket shape different. The
edges contours alter and these can be extended by additional outcropping (beyond the innominate) bone graft. Not really a shelf. This method is a subset of both the S.L.O.B. and the Cafe' Door procedures (though more extensive in the former).
|